

Predictive value of combined DCE-MRI perfusion parameters and clinical features nomogram for microsatellite instability in colorectal cancer
- PMID: 40410525
- PMCID: PMC12102045
- DOI: 10.1007/s12672-025-02705-x
Predictive value of combined DCE-MRI perfusion parameters and clinical features nomogram for microsatellite instability in colorectal cancer
Abstract
Objectives: To develop a nomogram that combines dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) perfusion parameters, ADC values and clinical features to preoperatively identify microsatellite instability (MSI) in patients with colorectal cancer (CRC).
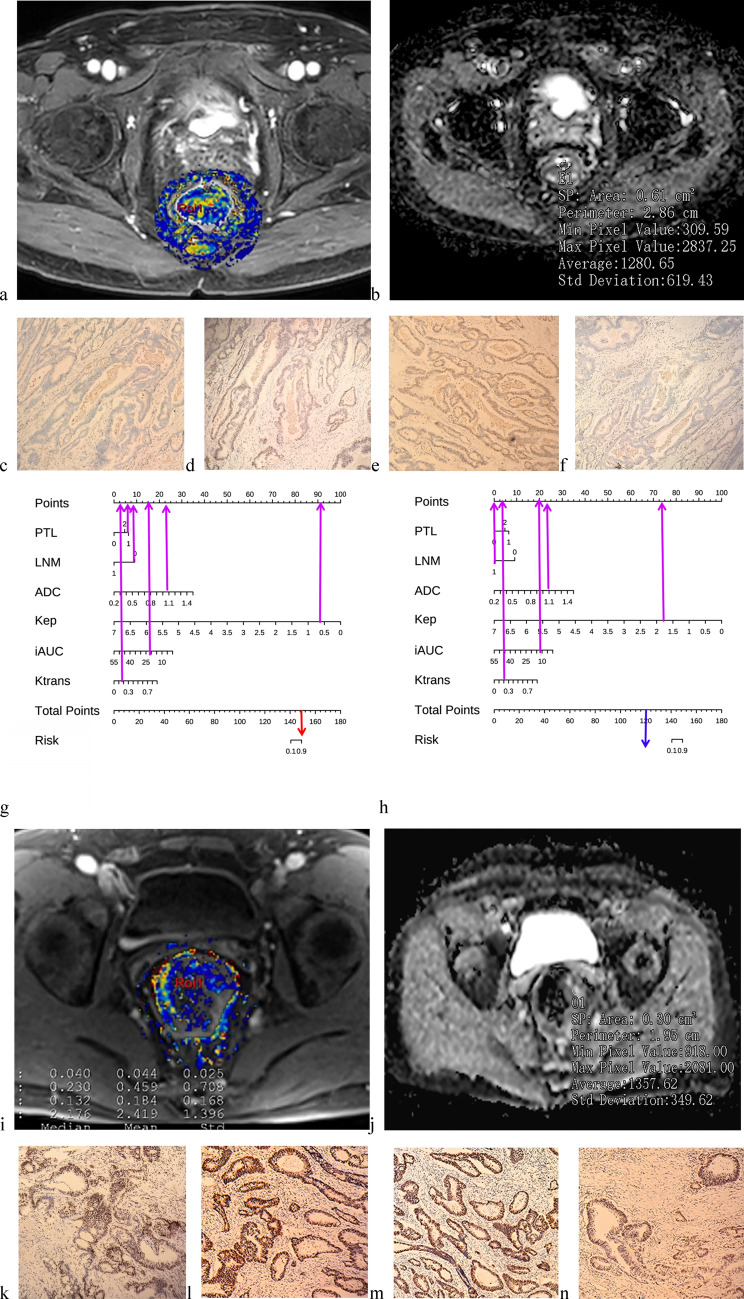
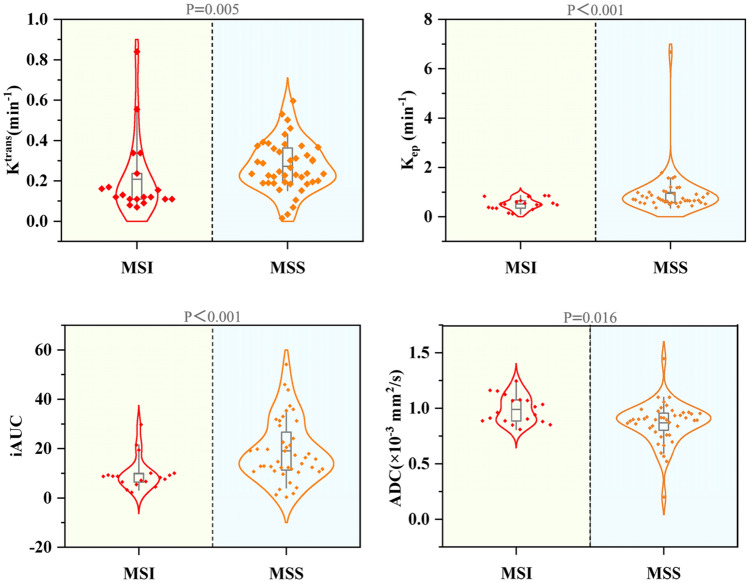
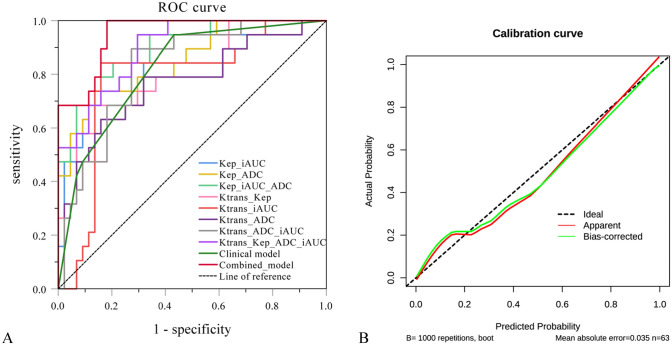
Methods: This retrospective study included 63 CRC patients who underwent preoperative DCE-MRI and had immunohistochemistry results available. Two radiologists, in a double-blind manner, placed two circular regions of interests in the area with the highest perfusion intensity on the DCE-MRI perfusion map and the corresponding area on the ADC map. Perfusion parameters and ADC values were measured, and the average values from both radiologists were used for subsequent analysis. Univariate analysis was performed to identify independent risk factors for MSI. A nomogram was then constructed by combining the most significant clinical risk factors with DCE-MRI perfusion parameters. The model's performance was evaluated using receiver operating characteristic (ROC) curves. Calibration curves, decision curve analysis (DCA), and clinical impact curves (CIC) were used to assess the nomogram's clinical utility and net benefit.
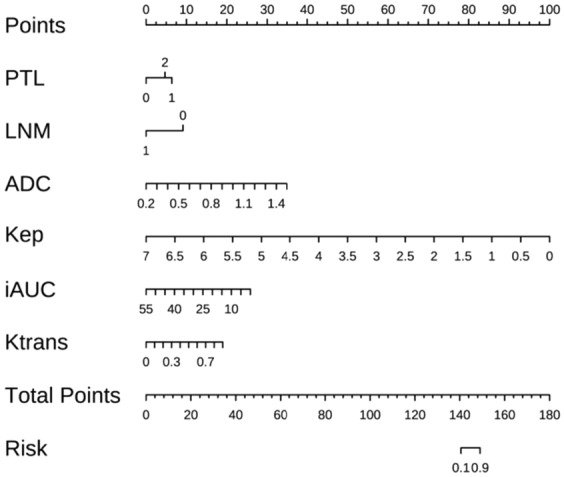
Results: The nomogram prediction model, which combined PLT, LNM, Ktrans, Kep, iAUC, and ADC, demonstrated good predictive performance. The combined model had an AUC of 0.951 (95% CI: 0.903-0.998), an accuracy of 0.873, a sensitivity of 1.000, and a specificity of 0.818. Both the DCA and CIC demonstrated good clinical applicability and net benefit.
Conclusion: The nomogram method demonstrated good potential in the preoperative individualized identification of MSI status in CRC patients. This tool can assist clinicians in adopting appropriate treatment strategies and optimizing personalized stratification for CRC patients.
Keywords: Colorectal cancer; DCE; Magnetic resonance imaging; Microsatellite instability; Nomogram.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: The study was approved by the Ethics Review Committee of Gansu Provincial Hospital (no. 2023-725). We confirm that all experiments were conducted in accordance with relevant guidelines and regulations. Although this study does not involve animal experiments, we have adhered to the ARRIVE guidelines ( https://arriveguidelines.org ) to ensure that the methodology is fully evaluable and reproducible. Consent to participate: All the authors have followed the applicable ethical standards to maintain the research integrity without any duplication, fraud or plagiarism issues. This study had the consent of all human participants, and all co-authors reviewed the manuscript and agreed to publish the study. Consent for publication: Not applicable. Competing interests: The authors declare that they are no competing interests in this study.
Figures



References
-
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–63. - PubMed
-
- Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394:1467–80. - PubMed
-
- Ribic CM, Sargent DJ, Moore MJ, Thibodeau SN, French AJ, Goldberg RM, Hamilton SR, Laurent-Puig P, Gryfe R, Shepherd LE, et al. Tumor microsatellite-instability status as a predictor of benefit from fluorouracil-based adjuvant chemotherapy for colon cancer. N Engl J Med. 2003;349:247–57. - PMC - PubMed
Grants and funding
- No. 2025CXCY-071/Gansu Provincial Department of Education: Graduate Student "Innovation and Entrepreneurship" Project of Gansu University of Chinese Medicine
- No.23GSSYA-2/Gansu Provincial Hospital Research Fund Project
- No.23GSSYF-4/Gansu Provincial Hospital Research Fund Project
- No.20JR5RA143/Gansu Provincial Youth Science and Technology Fund Project
LinkOut - more resources
Full Text Sources
Miscellaneous