

How to approach a patient hospitalized for pneumonia who is not responding to treatment?
- PMID: 40411623
- PMCID: PMC12129858
- DOI: 10.1007/s00134-025-07903-3
How to approach a patient hospitalized for pneumonia who is not responding to treatment?
Erratum in
-
Correction: How to approach a patient hospitalized for pneumonia who is not responding to treatment?Intensive Care Med. 2025 Aug;51(8):1570-1571. doi: 10.1007/s00134-025-08027-4. Intensive Care Med. 2025. PMID: 40658251 Free PMC article. No abstract available.
Abstract
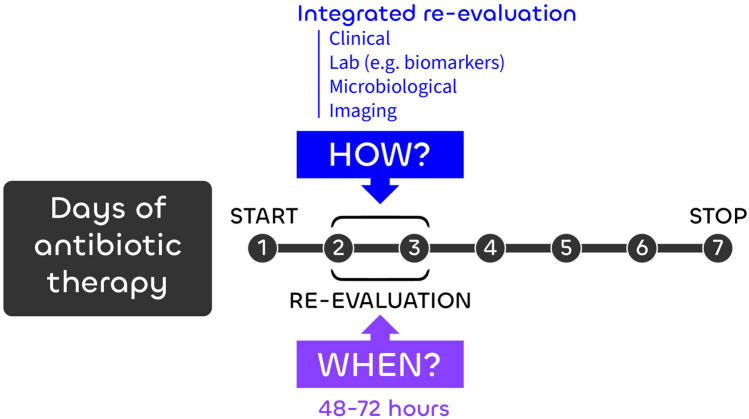
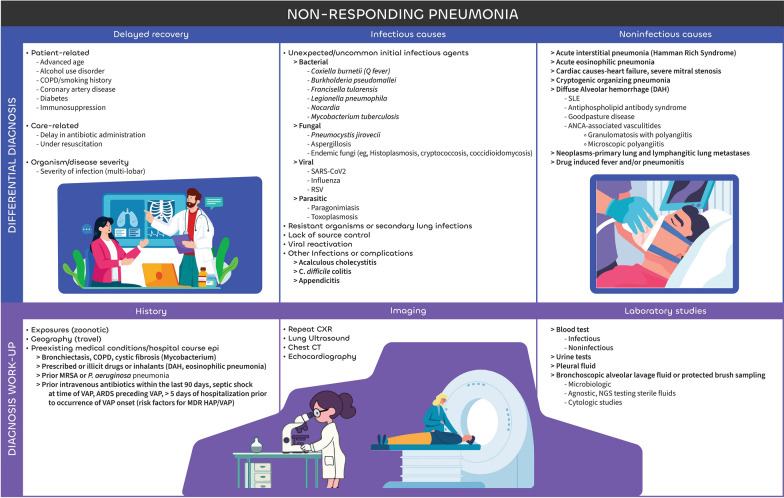
Pneumonia is a frequent cause of intensive care unit (ICU) admission and is the most common infection in ICU patients across all geographic regions. It takes 48-72h for most patients to respond to appropriate antibiotic therapy. Non-response is typically defined as the persistence/worsening of clinical signs-such as fever, respiratory distress, impaired oxygenation and/or radiographic abnormalities-with rates ranging 20-30%. Several factors can contribute to non-response. Host factors, including immunosuppression, chronic lung disease, or ongoing aspiration, may impair resolution. Additionally, incorrect antibiotic dosing, atypical or resistant pathogens (such as multidrug-resistant bacteria, Mycobacterium tuberculosis, or fungal infections) may be responsible, requiring alternative antimicrobial strategies. A septic complication related to pneumonia (e.g., empyema) or not (e.g., acalculous cholecystitis) may need to be excluded. Finally, non-infectious conditions (e.g., pulmonary embolism, malignancy, secondary ARDS or vasculitis) that can mimic or potentiate pneumonia must be considered. Although non-responding pneumonia is frequent, its management lacks strong evidence, and its approach is based mostly on the art of medicine and clinical judgement. Clinicians should continuously reassess the medical history and physical exam, review microbiological data, and consider imaging such as chest CT. Bronchoscopy or repeat sputum sampling may aid in identifying alternative pathogens or non-infectious causes. The management of a non-responding pneumonia depends on the findings of a structured reassessment. Herein, we provide guidance on how to identify and manage non-responding pneumonia. Ultimately, addressing pneumonia that does not respond to antibiotics is crucial for preventing complications, optimizing antimicrobial stewardship, and improving patient outcomes.
Keywords: Community-acquired pneumonia; Hospital-acquired pneumonia; Management; Nonresponding pneumonia; Pneumonia; Ventilator-associated pneumonia.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: PP received fees for lecture from Gilead and Mundipharma, consulting from MSD and Biocodex. KC received fees for lectures and advisory board from BD. RF received fees as speaker and/or advisor for Pfizer, MSD, Shionogi, Gilead, GE, AOP Health, Grifols, Thermofisher, Estor, Toray, BD, Menarini, Viatris. CAG received consultation fees from Karius Inc Diagnostics. MK has grants from CDC, AHRQ; contracts from Massachusetts Department of Public Health; royalties from UpToDate. IML received fees lectures and advisory board MSD, Menarini, Biomerieux, Mundipharma, Gilead, and Thermofisher. SN received consultation fees from Mundipharma, and lecture fees from MSD, Biomérieux, Pfizer, Fisher and Peykel, Shionogi, and Medtronic. LC, JC, SEC, TL, JIFS, SS, DS, AK declare no conflict of interest.
Figures
References
-
- Halm EA, Fine MJ, Marrie TJ et al (1998) Time to clinical stability in patients hospitalized with community-acquired pneumonia: implications for practice guidelines. JAMA 279:1452–1457. 10.1001/jama.279.18.1452 - PubMed
-
- Arancibia F, Ewig S, Martinez JA et al (2000) Antimicrobial treatment failures in patients with community-acquired pneumonia: causes and prognostic implications. Am J Respir Crit Care Med 162:154–160. 10.1164/ajrccm.162.1.9907023 - PubMed
-
- Roson B, Carratala J, Fernandez-Sabe N et al (2004) Causes and factors associated with early failure in hospitalized patients with community-acquired pneumonia. Arch Intern Med 164:502–508. 10.1001/archinte.164.5.502 - PubMed
