

Enhanced staging of renal cell carcinoma using tumor morphology features: model development and multi-source validation
- PMID: 40413285
- PMCID: PMC12103548
- DOI: 10.1038/s41746-025-01723-x
Enhanced staging of renal cell carcinoma using tumor morphology features: model development and multi-source validation
Abstract
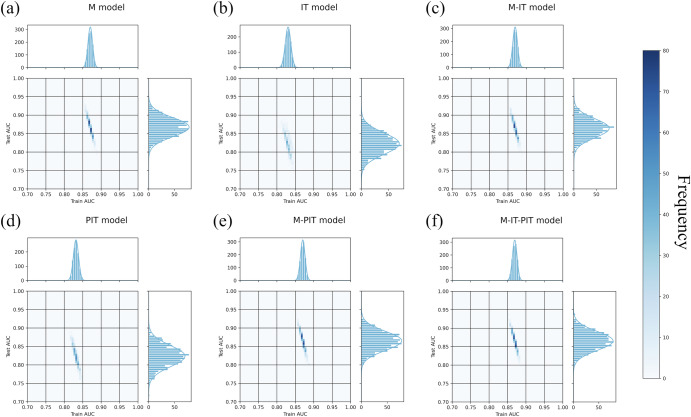
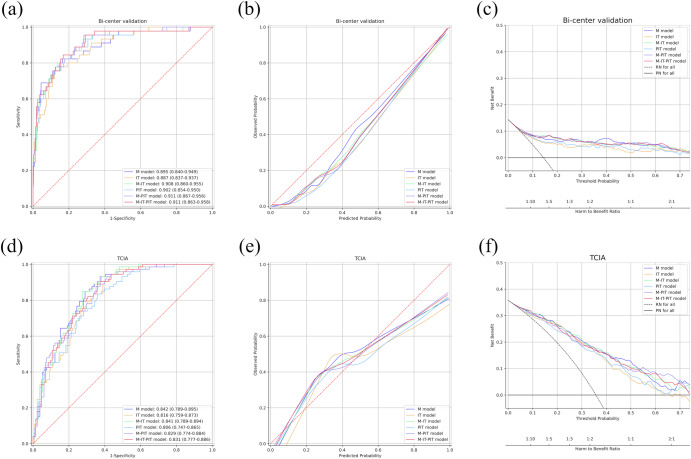
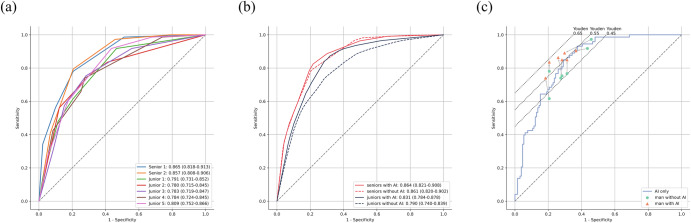
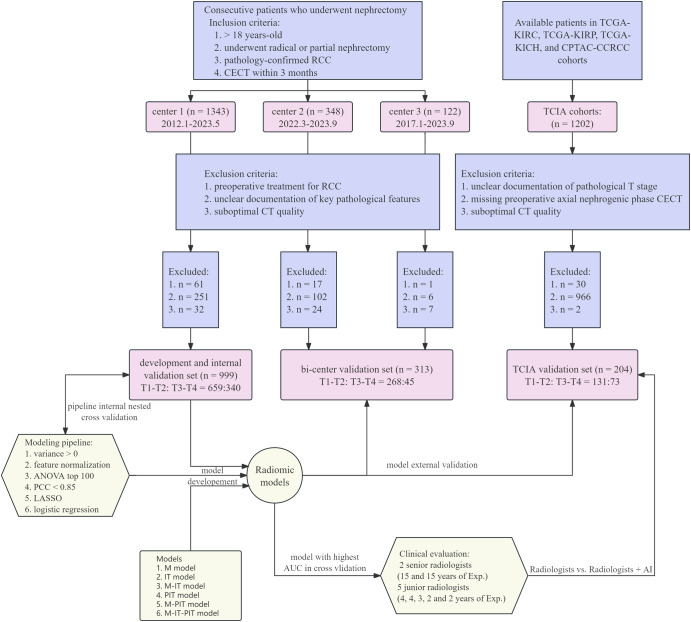
Preoperative detection of pT3a invasion in non-metastatic renal cell carcinoma (RCC) remains challenging with CT. This study developed and validated radiomic models using preoperative CT to identify pT3a invasions. Six models were trained and internally validated via nested cross-validation on 999 patients from one hospital. External validation included 313 patients from two hospitals and 204 patients from four TCIA datasets. A multi-reader multi-case study with seven radiologists evaluated the model's incremental value. The morphology model achieved the highest internal AUC (0.867, 95% CI: 0.866-0.869) and maintained performance in external validations (AUC = 0.895 and 0.842). When used as a second reader, it significantly improved junior radiologists' sensitivity and discrimination (AUC: 0.790 vs. 0.831, p < 0.001) without compromising specificity. This study demonstrates that CT-based radiomic models, particularly the morphology model, can reliably detect pT3a invasion and enhance diagnostic accuracy for junior radiologists, offering potential clinical utility in preoperative staging.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures

References
-
- Ljungberg, B. et al. European Association of Urology Guidelines on renal cell carcinoma: the 2022 update. Eur. Urol.82, 399–410 (2022). - PubMed
-
- Johnson, C. D., Dunnick, N. R., Cohan, R. H. & Illescas, F. F. Renal adenocarcinoma: CT staging of 100 tumors. Am. J. Roentgenol.148, 59–63 (1987). - PubMed
-
- Türkvatan, A. et al. Preoperative staging of renal cell carcinoma with multidetector CT. Diagn. Interv. Radiol.15, 22–30 (2009). - PubMed
-
- Liu, Y., Song, T., Huang, Z., Zhang, S. & Li, Y. The accuracy of multidetector computed tomography for preoperative staging of renal cell carcinoma. Int. Braz. J. Urol.38, 627–636 (2012). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
