

Impact of RSV infection on mortality, rehospitalization, and long-term pulmonary, cardiovascular, and functional outcomes in hospitalized adults: a systematic review and meta-analysis
- PMID: 40413443
- PMCID: PMC12103016
- DOI: 10.1186/s12985-025-02785-9
Impact of RSV infection on mortality, rehospitalization, and long-term pulmonary, cardiovascular, and functional outcomes in hospitalized adults: a systematic review and meta-analysis
Abstract
Background: Respiratory syncytial virus (RSV) is increasingly recognized as a significant pathogen in adults, particularly those with underlying comorbidities. However, the burden of RSV on post-hospital outcomes remains underexplored. This study aimed to assess the impact of RSV infection on mortality, rehospitalization, and long-term pulmonary, cardiovascular, and functional outcomes in hospitalized adults.
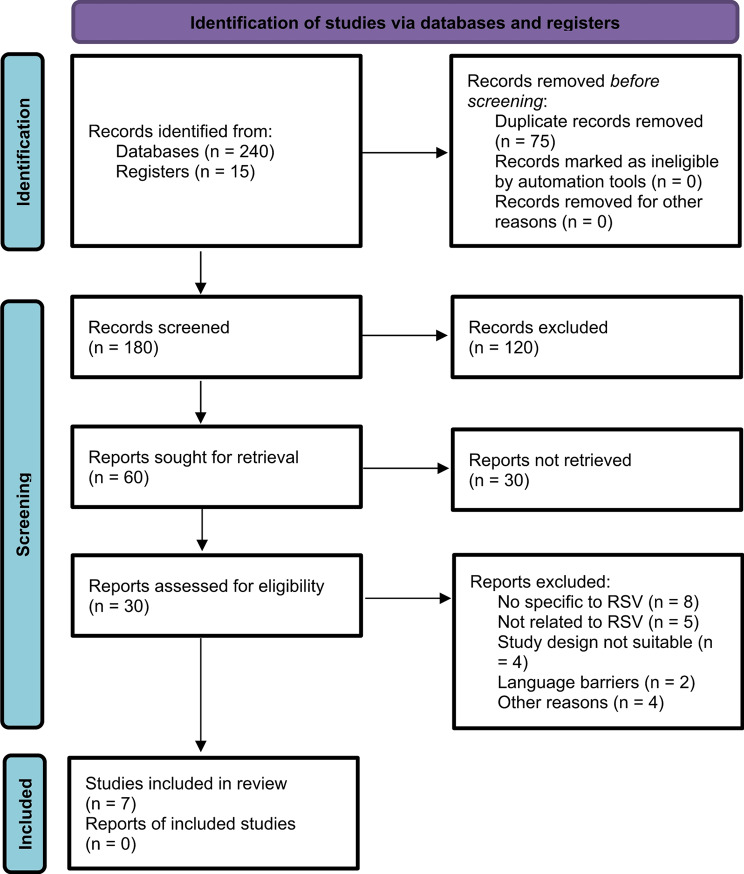
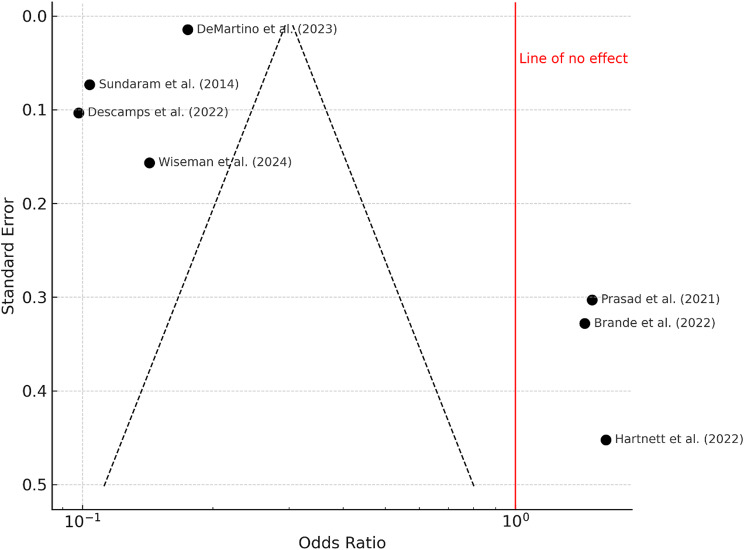
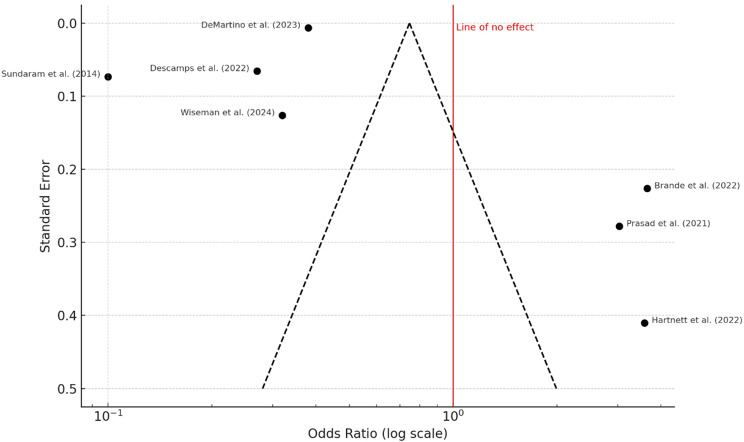
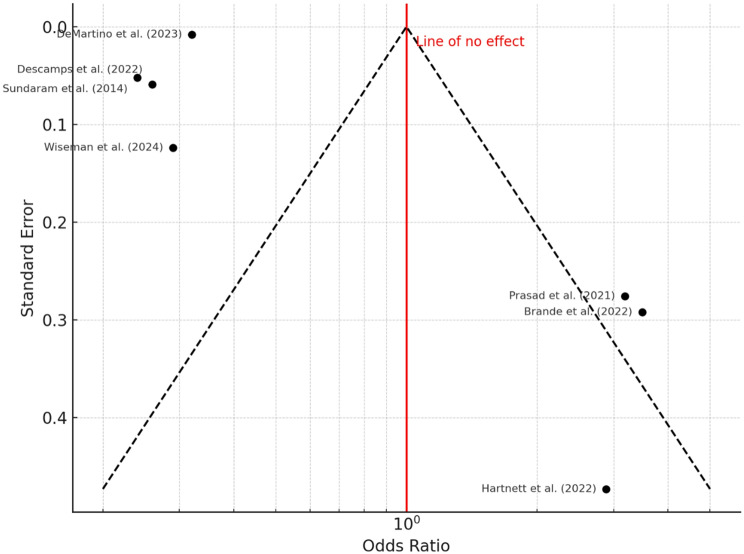
Methods: A systematic review and meta-analysis were conducted according to PRISMA 2020 guidelines. A comprehensive search of major databases until February 2025 identified cohort and observational studies reporting on clinical outcomes in adults with laboratory-confirmed RSV infection. A total of seven eligible studies encompassing 180,125 patients were included. Pooled odds ratios (OR) with 95% confidence intervals (CI) were calculated using a random-effects model. The risk of bias was assessed using the Newcastle-Ottawa Scale and the ROBINS-I tool. Funnel plots and Egger's test were used to assess publication bias.
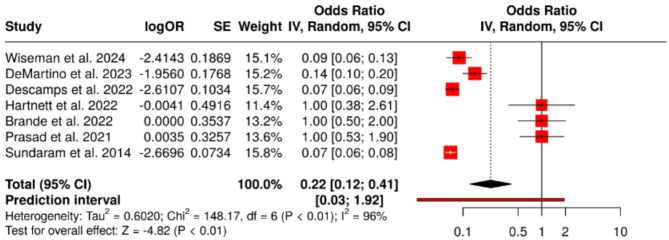
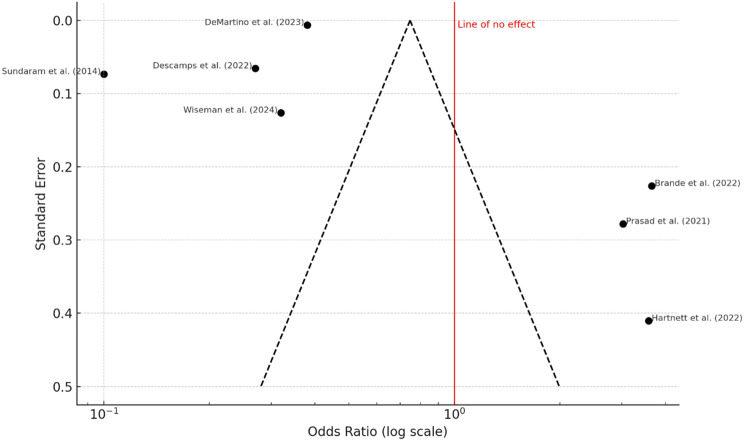
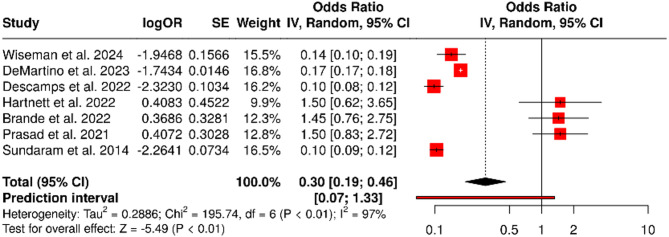
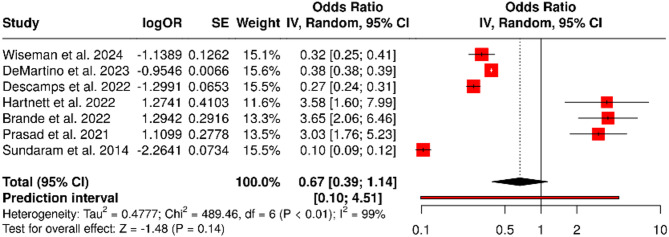
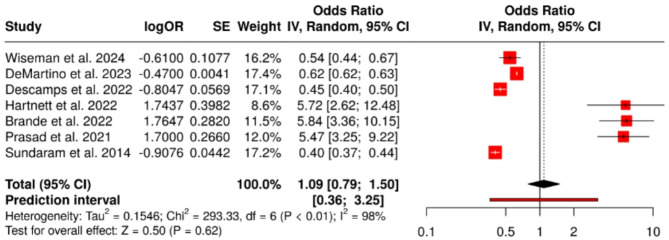
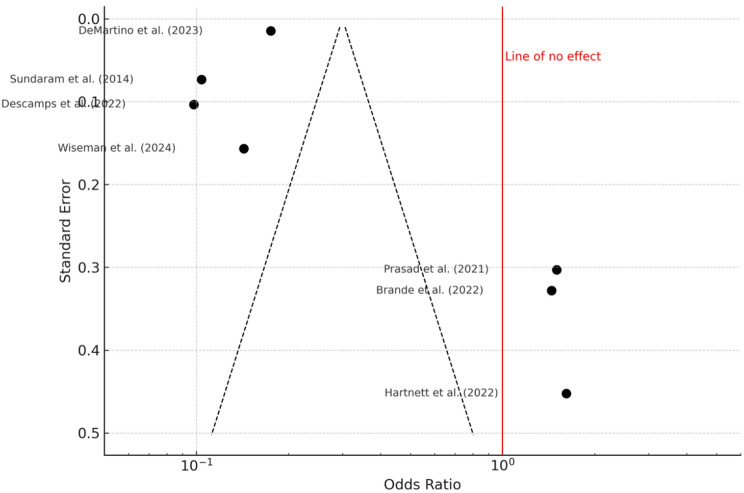
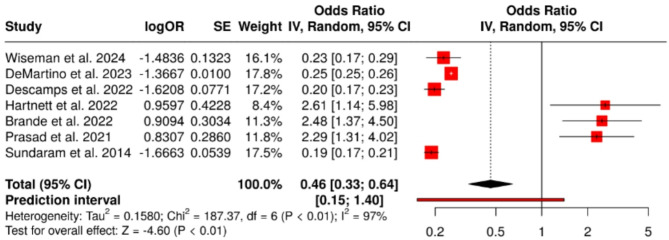
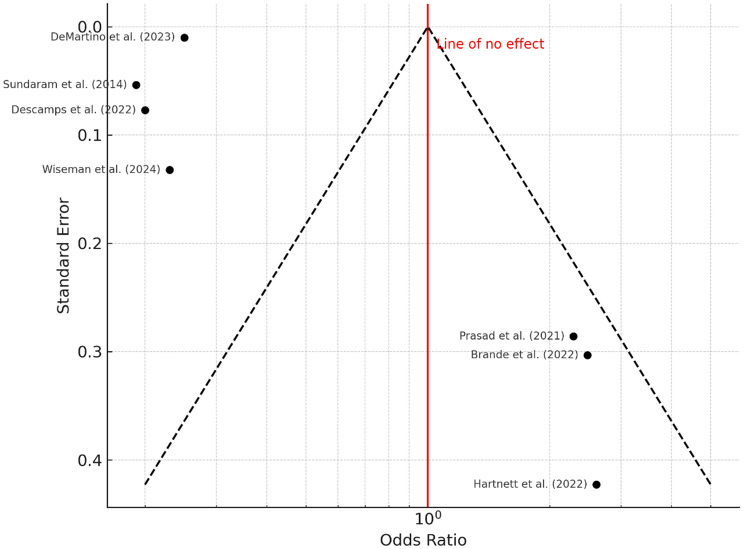
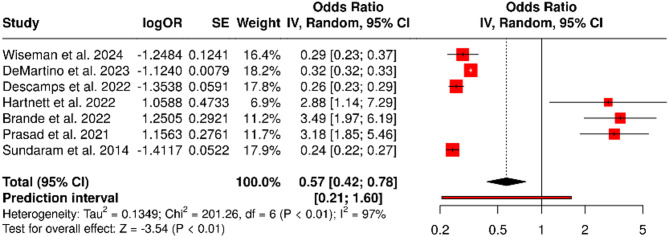
Results: RSV infection was associated with significantly increased 30-day mortality (OR 0.22, 95% CI: 0.12-0.41; P < 0.01, I² = 96%) and 90-day mortality (OR 0.30, 95% CI: 0.19-0.46; P < 0.01, I² = 97%). Although the odds ratios are below 1, this indicates higher mortality in RSV-positive patients, as the reference groups had lower risk. Statistically significant associations were also found for cardiovascular complications (OR 0.46, 95% CI: 0.33-0.64) and functional impairments (OR 0.57, 95% CI: 0.42-0.78). No significant association was identified for 90-day rehospitalization (OR 0.67, 95% CI: 0.39-1.14) or pulmonary impairments (OR 1.09, 95% CI: 0.79-1.50). Heterogeneity was high across most outcomes. Publication bias was only evident for the 30-day mortality outcome.
Conclusions: RSV infection in hospitalized adults is associated with elevated short- and medium-term mortality, as well as increased risk of cardiovascular and functional complications post-discharge. These findings highlight the need for RSV-specific prevention strategies, including vaccination and post-acute care planning, particularly for vulnerable adult populations.
Clinical trial number: Not applicable.
Keywords: Cardiovascular events; Functional decline; Mortality; Pulmonary impairments; RSV infection; Rehospitalization.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval and consent to participate: This study is a systematic review and meta-analysis based exclusively on previously published data. No new data involving human participants were collected or analyzed. Therefore, ethical approval and informed consent were not required. Consent to publish: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Cardiac Events in Adults Hospitalized for Respiratory Syncytial Virus vs COVID-19 or Influenza.JAMA Netw Open. 2025 May 1;8(5):e2511764. doi: 10.1001/jamanetworkopen.2025.11764. JAMA Netw Open. 2025. PMID: 40402498 Free PMC article.
-
Acute Cardiac Events in Hospitalized Older Adults With Respiratory Syncytial Virus Infection.JAMA Intern Med. 2024 Jun 1;184(6):602-611. doi: 10.1001/jamainternmed.2024.0212. JAMA Intern Med. 2024. PMID: 38619857 Free PMC article.
-
High bacterial coinfection rates and associated mortality among hospitalized older adults with laboratory-confirmed respiratory syncytial virus infection.J Microbiol Immunol Infect. 2025 Aug;58(4):422-428. doi: 10.1016/j.jmii.2025.03.005. Epub 2025 Mar 17. J Microbiol Immunol Infect. 2025. PMID: 40118719
-
Acute Lower Respiratory Infections Associated With Respiratory Syncytial Virus in Children With Underlying Congenital Heart Disease: Systematic Review and Meta-analysis.J Infect Dis. 2020 Oct 7;222(Suppl 7):S613-S619. doi: 10.1093/infdis/jiz150. J Infect Dis. 2020. PMID: 31599958
-
Global disease burden of and risk factors for acute lower respiratory infections caused by respiratory syncytial virus in preterm infants and young children in 2019: a systematic review and meta-analysis of aggregated and individual participant data.Lancet. 2024 Mar 30;403(10433):1241-1253. doi: 10.1016/S0140-6736(24)00138-7. Epub 2024 Feb 14. Lancet. 2024. PMID: 38367641
References
-
- Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratory syncytial virus infection in elderly and high-risk adults. Am J Respir Crit Care Med. 2005;171(3):250–5. 10.1164/rccm.200410-1406OC. - PubMed
-
- Shi T, Denouel A, Tietjen AK, Campbell I, Moran E, Li X, et al. Global disease burden estimates of respiratory syncytial virus-associated acute respiratory infection in older adults in 2015: A systematic review and meta-analysis. Lancet. 2020;396(10242):685–700. 10.1016/S0140-6736(19)32989-7. - PubMed
-
- Nichols MK, Andrew MK, Hatchette TF, McNeil SA. Epidemiology of respiratory syncytial virus infection in older adults: A systematic review of cohort and case-control studies. Clin Infect Dis. 2021;73(6):e1567–78. 10.1093/cid/ciab243.
-
- Walsh EE, Peterson DR, Falsey AR. Risk factors for severe respiratory syncytial virus infection in elderly persons. J Infect Dis. 2013;208(10):1736–46. 10.1164/rccm.201212-2220OC. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
