

The aggregate index of systemic inflammation (AISI) and the risk of all-cause, cardiovascular, and cardio-cerebrovascular mortality in congestive heart failure patients: results from NHANES 1999-2018
- PMID: 40414913
- PMCID: PMC12104397
- DOI: 10.1038/s41598-025-01196-8
The aggregate index of systemic inflammation (AISI) and the risk of all-cause, cardiovascular, and cardio-cerebrovascular mortality in congestive heart failure patients: results from NHANES 1999-2018
Abstract
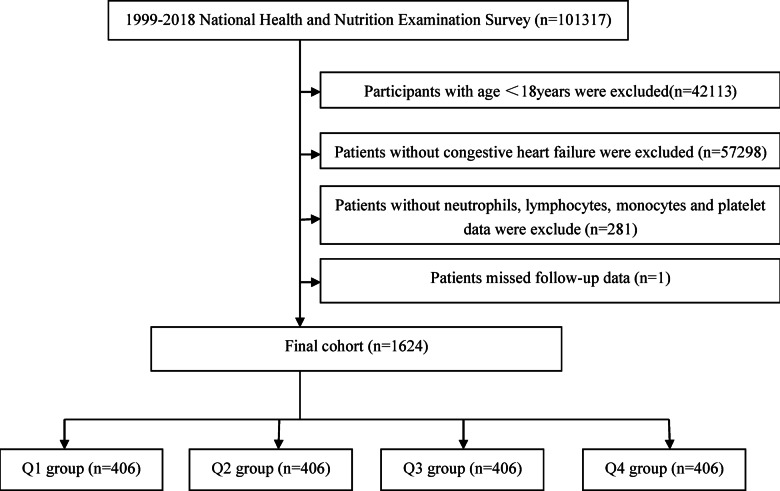
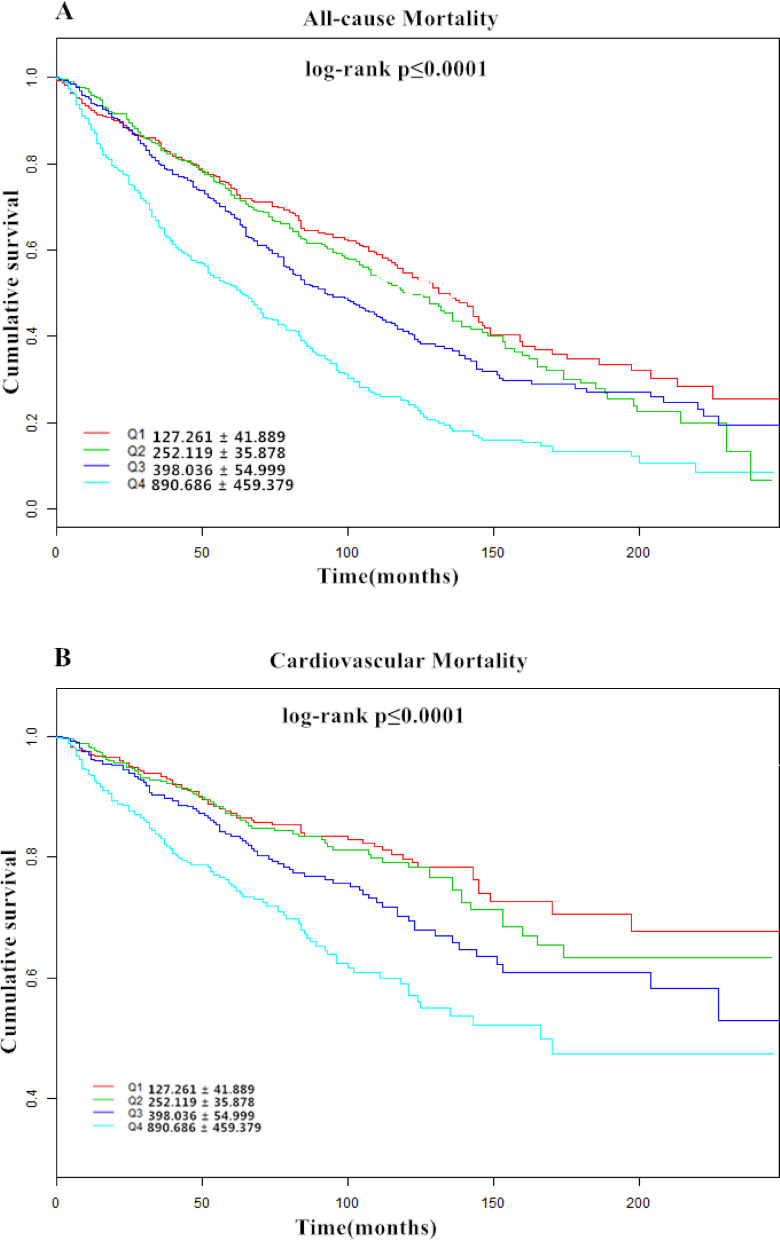
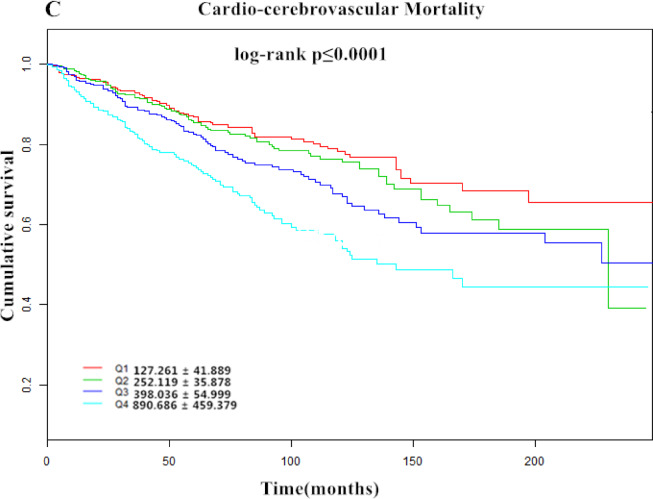
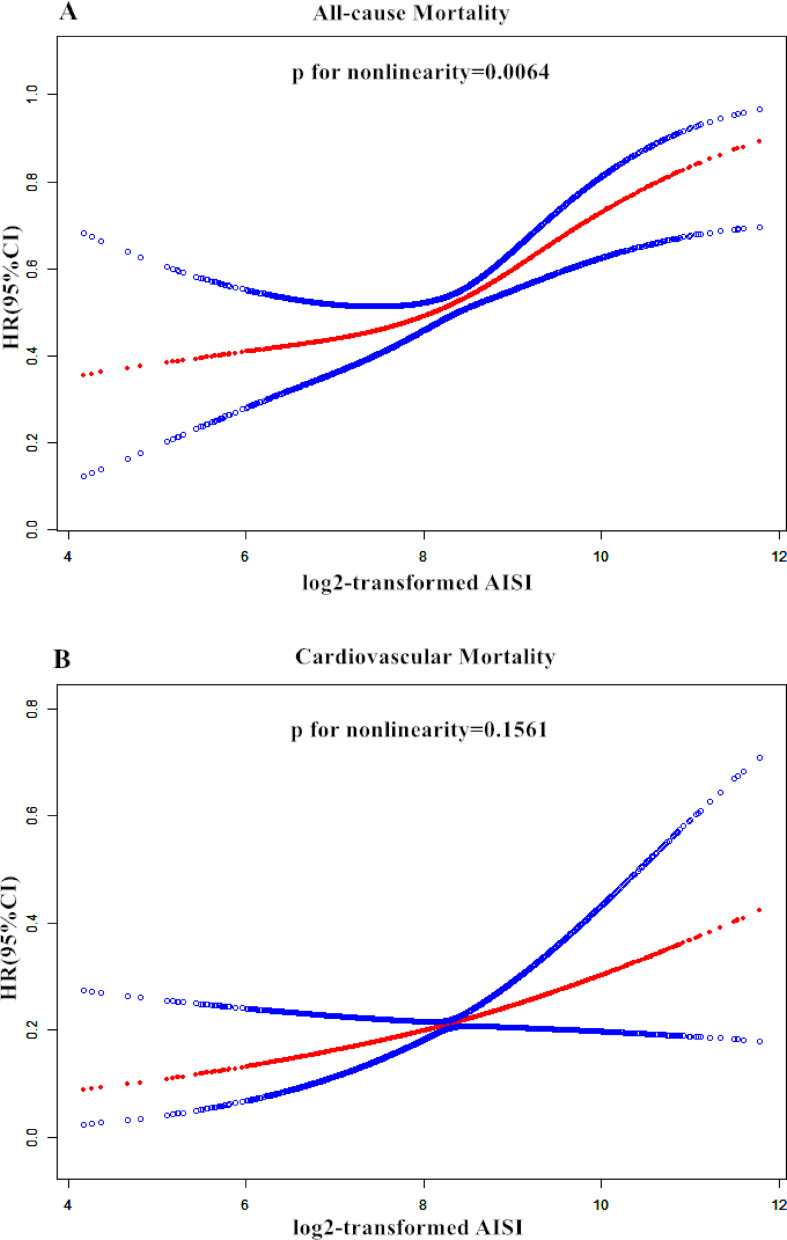
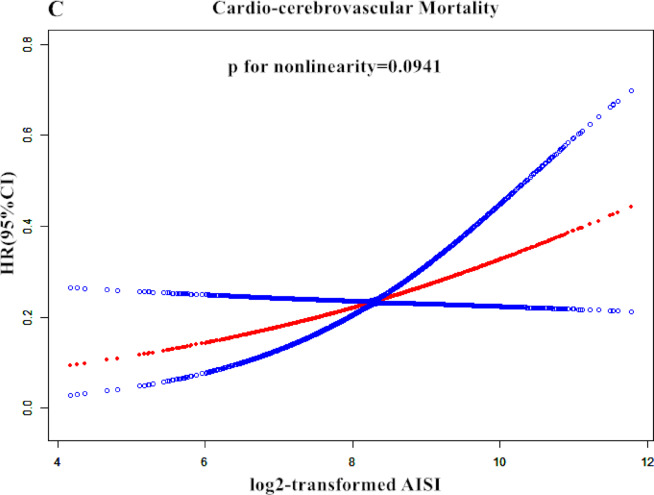
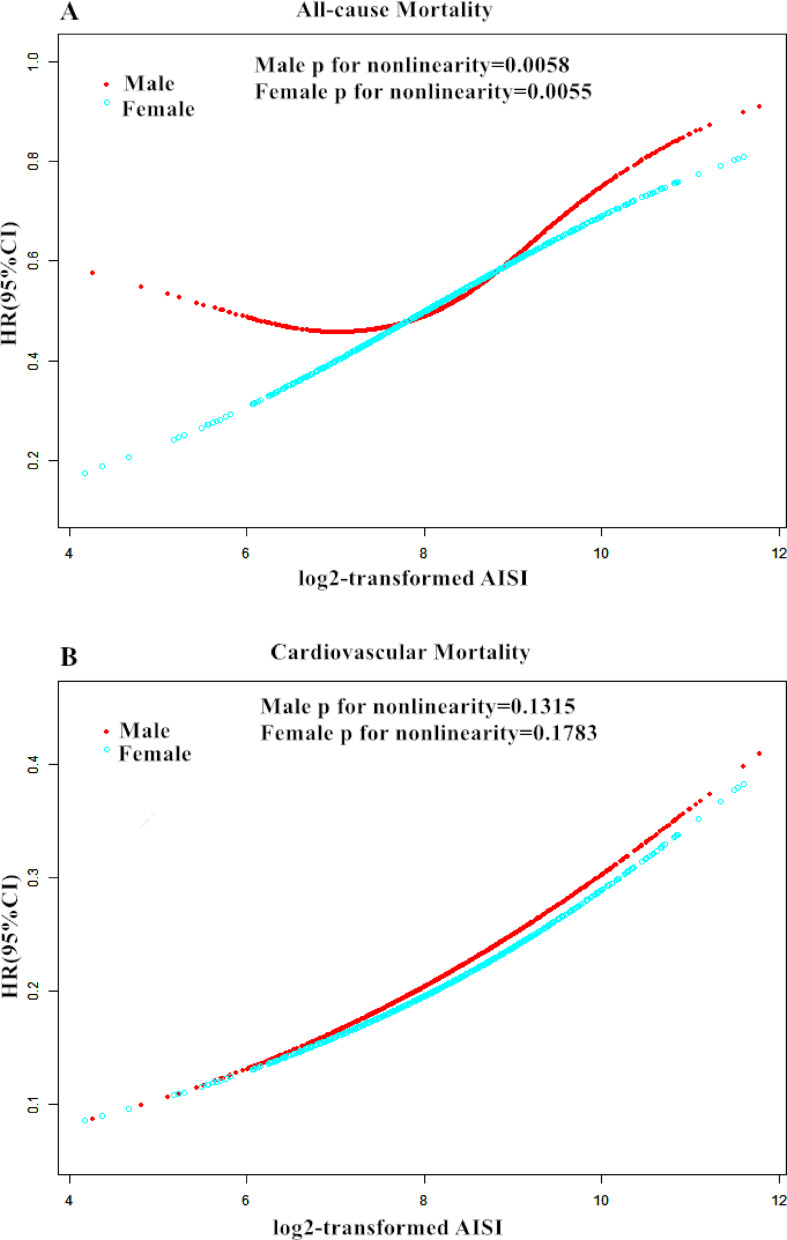
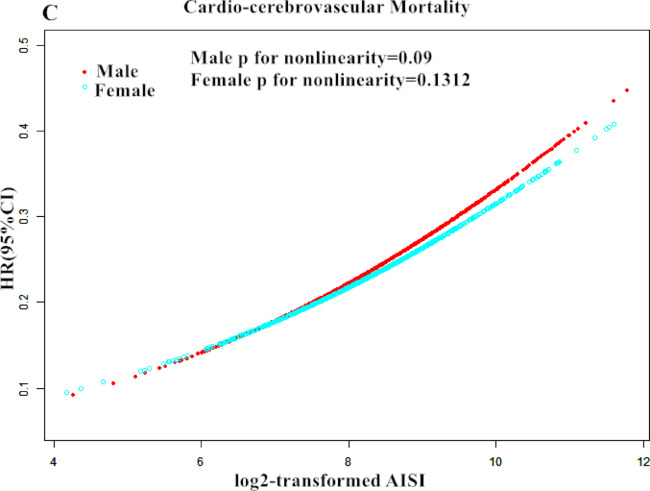
Congestive heart failure (CHF) is a prevalent cardiovascular disease, with increasing incidence and mortality rates associated with aging populations and rising rates of chronic diseases. Systemic inflammatory response is recognized to play a pivotal role in the pathogenesis of CHF, and the aggregate index of systemic inflammation (AISI) has garnered widespread attention as a comprehensive indicator reflecting inflammatory status in recent years. However, there is currently a lack of large-scale epidemiological studies investigating the relationship between AISI and all-cause, cardiovascular, and cardio-cerebrovascular mortality risks among CHF patients. This study aims to utilize data from the NHANES database spanning 1999 to 2018 to analyze the association between AISI and prognosis in CHF patients, aiming to provide new evidence to support research into the pathophysiology and clinical management of CHF. This study enrolled 1624 patients aged ≥ 18 years with congestive heart failure (CHF) from the National Health and Nutrition Examination Survey spanning 1999 to 2018. Patients were stratified into four groups based on the aggregate index of systemic inflammation (AISI). Survival differences among the groups were compared using log-rank tests and Kaplan-Meier curves. Additionally, multivariable Cox regression and restricted cubic spline analyses were employed to explore the relationship between AISI and all-cause, cardiovascular, and cardio-cerebrovascular mortality. Overall, during a mean follow-up of 76.4 ± 56.6 months among patients with congestive heart failure, a total of 828 participants (51.042%) died. Among these, 314 (19.389%) deaths were attributed to cardiovascular diseases, and 344 (21.226%) were related to cardio-cerebrovascular mortality. Kaplan-Meier analysis revealed significant differences in all-cause, cardiovascular, and cardio-cerebrovascular mortality among AISI quartiles (log-rank test: all P < 0.001). Multivariable adjusted models demonstrated that participants in the highest AISI quartile had increased risks of all-cause mortality (hazard ratio [HR] = 1.599, 95% confidence interval [CI] 1.595-1.602), cardiovascular mortality (HR = 1.070, 95% CI 1.066-1.074), and cardio-cerebrovascular mortality (HR = 1.173, 95% CI 1.168-1.177) compared to those in the lowest quartile. Additionally, restricted cubic spline analysis indicated a nonlinear association between AISI and all-cause mortality (P = 0.0064), with an inflection point at AISI 8.66. On the left flank of the inflection point, each twofold increase in AISI was associated with a 19.6% higher risk of all-cause mortality (HR = 1.196, 95% CI 0.930-1.538), while on the right flank, there was a 126.2% increase (HR = 2.262, 95% CI 1.506-3.395). Furthermore, each twofold change in AISI was nonlinearly associated with a 60.2% higher risk of cardiovascular mortality (HR = 1.602, 95% CI 1.075-2.388) and a 56.6% higher risk of cardio-cerebrovascular mortality (HR = 1.566, 95% CI 1.072-2.286). E-value analysis suggested robustness to unmeasured confounding. In the population of patients with congestive heart failure aged 18 years and older in the United States, irrespective of established risk factors, AISI was significantly associated with all-cause, cardiovascular, and cardio-cerebrovascular mortality. Further research is needed to validate this.
Keywords: All-cause mortality; Cardio-cerebrovascular mortality; Cardiovascular mortality; NHANES; The aggregate index of systemic inflammation AISI.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: The ethics review board of the National Center for Health Statistics approved all NHANES protocols and written informed consents were obtained from all participants.
Figures
Similar articles
-
Relationship between aggregate index of systemic inflammation and mortality from CCD and malignant neoplasms in diabetic patients.Sci Rep. 2025 Jul 22;15(1):26545. doi: 10.1038/s41598-025-12094-4. Sci Rep. 2025. PMID: 40696035 Free PMC article.
-
Systemic immune-inflammation index (SII) and the risk of all-cause, cardiovascular, and cardio-cerebrovascular mortality in the general population.Eur J Med Res. 2023 Dec 9;28(1):575. doi: 10.1186/s40001-023-01529-1. Eur J Med Res. 2023. PMID: 38066657 Free PMC article.
-
Association of systemic immune-inflammation index with all-cause and cardio-cerebrovascular mortality in individuals with diabetic kidney disease: evidence from NHANES 1999-2018.Front Endocrinol (Lausanne). 2024 Nov 26;15:1399832. doi: 10.3389/fendo.2024.1399832. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39659615 Free PMC article.
-
[Association Between the Aggregate Index of Systemic Inflammation and Albuminuria: A Cross-Sectional Study of National Health and Nutrition Examination Survey 2007-2018].Sichuan Da Xue Xue Bao Yi Xue Ban. 2024 May 20;55(3):671-679. doi: 10.12182/20240560108. Sichuan Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 38948283 Free PMC article. Chinese.
-
Association of Life's essential 8 score with the risk of all-cause mortality and cardio-cerebrovascular mortality in patients with stroke.BMC Cardiovasc Disord. 2024 Jun 25;24(1):320. doi: 10.1186/s12872-024-03947-3. BMC Cardiovasc Disord. 2024. PMID: 38918724 Free PMC article.
Cited by
-
Relationship between aggregate index of systemic inflammation and mortality from CCD and malignant neoplasms in diabetic patients.Sci Rep. 2025 Jul 22;15(1):26545. doi: 10.1038/s41598-025-12094-4. Sci Rep. 2025. PMID: 40696035 Free PMC article.
-
Inflammatory indices AISI and SIRI in atherosclerosis risk stratification: validation across community and intensive care populations.Ann Med. 2025 Dec;57(1):2530792. doi: 10.1080/07853890.2025.2530792. Epub 2025 Jul 13. Ann Med. 2025. PMID: 40652407 Free PMC article.
References
-
- Heidenreich, P. A. et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: A report of the American college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation145 (18), e876–e894. 10.1161/CIR.0000000000001062 (2022). Epub 2022 Apr 1. PMID: 35363500. - PubMed
-
- Xia, Y. et al. Systemic immune inflammation index (SII), system inflammation response index (SIRI) and risk of All-Cause mortality and cardiovascular mortality: A 20-Year Follow-Up cohort study of 42,875 US adults. J. Clin. Med.12 (3), 1128. 10.3390/jcm12031128 (2023). PMID: 36769776; PMCID: PMC9918056. - PMC - PubMed
-
- Haneuse, S. VanderWeele TJ,Arterburn d.using the e-value to assess the potential effect of unmeasured confounding in observational studies.jama.2019:321(6):602–603 .10.1001/jama.2018.21554 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
