

Anti-KIT Barzolvolimab for Chronic Spontaneous Urticaria
- PMID: 40415544
- PMCID: PMC12368744
- DOI: 10.1111/all.16598
Anti-KIT Barzolvolimab for Chronic Spontaneous Urticaria
Abstract
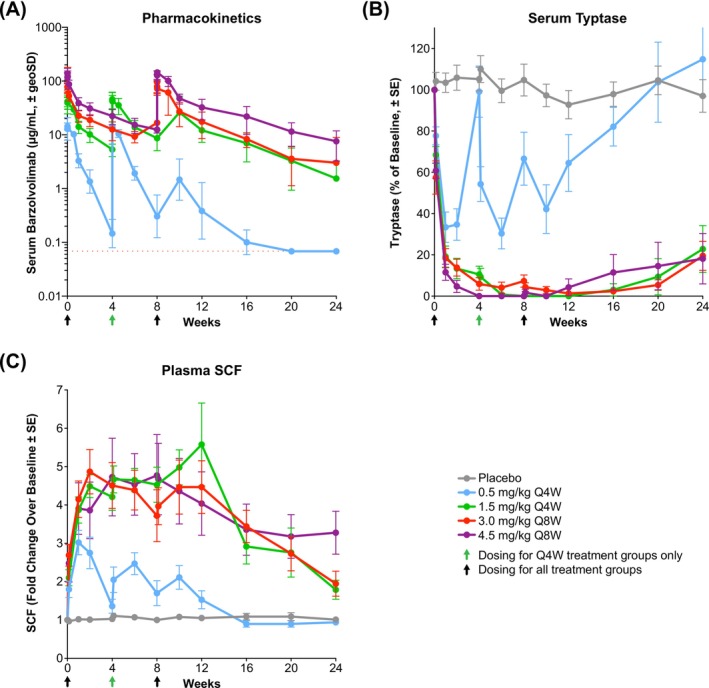
Background: Chronic spontaneous urticaria (CSU) is characterized by mast cell (MC)-mediated wheals and/or angioedema without identifiable triggers and is driven by MC activation. Barzolvolimab-a monoclonal anti-KIT antibody-depletes MCs by inhibiting activation of KIT by stem cell factor. We evaluated multiple ascending doses in patients with CSU.
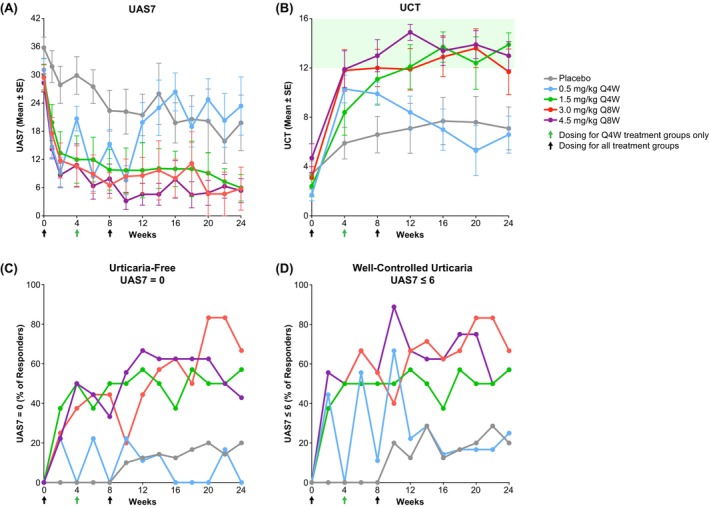
Methods: Phase 1b double-blind placebo-controlled trial (NCT04538794) in adults with moderate-to-severe (urticaria activity score over 7 days [UAS7] ≥ 16) antihistamine-refractory CSU treated with intravenous barzolvolimab for 12 weeks with a 12-week follow-up in four sequentially enrolled cohorts (randomized 4:1 barzolvolimab:placebo): 0.5 mg/kg, Q4W (n = 9); 1.5 mg/kg, Q4W (n = 8); 3 mg/kg, Q8W (n = 9); and 4.5 mg/kg, Q8W (n = 9). Primary and secondary objectives were safety and disease activity (UAS7 and urticaria control test [UCT]). Pharmacokinetics and pharmacodynamics were assessed.
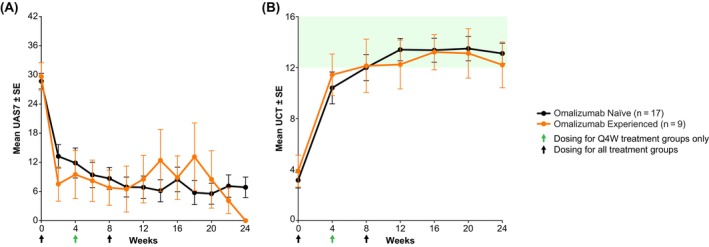
Results: Patients had high mean (range) baseline CSU activity, with UAS7 = 29.6 (16.3-42.0) for barzolvolimab-treated, UAS7 = 35.8 (19.0-42.0) for placebo-treated, and 44% prior omalizumab use. Multiple doses of barzolvolimab were well tolerated. Hair color change was the commonest adverse event in barzolvolimab-treated patients. Across barzolvolimab doses, rapid symptom reduction within 1 week was observed and sustained during 12 weeks; 71% of patients achieved a well-controlled (UAS7 ≤ 6) response and 57% a complete response (UAS7 = 0). Additionally, 77% of barzolvolimab-treated patients achieved a well-controlled response (UCT ≥ 12) and 43% a complete response (UCT = 16) by Week 12. The kinetics of disease activity paralleled tryptase suppression, indicative of MC inhibition. Patients with and without prior omalizumab treatment responded similarly.
Conclusions: This study supports barzolvolimab as a promising treatment for CSU.
Keywords: anti‐KIT; chronic urticaria; hives; mast cell; monoclonal antibody; stem cell factor.
© 2025 The Author(s). Allergy published by European Academy of Allergy and Clinical Immunology and John Wiley & Sons Ltd.
Conflict of interest statement
Diego Alvarado, Diane Young, Elizabeth Crowley, Elsa Paradise, Rick Ma, Thomas Hawthorne, and Margo Heath‐Chiozzi are full‐time employees of Celldex Therapeutics and may hold stock and/or stock options. Martin Metz reports being a speaker and/or advisor for AbbVie, Advanz, ALK Abello, Allegria, Almirall, Amgen, AstraZeneca, Argenx, Astria, Attovia, Berlin‐Chemie, Celldex, Celltrion, DeepApple, Escient, Galderma, GSK, Incyte, Jasper, Lilly, Novartis, Pfizer, Regeneron, Sanofi, Santa Ana Bio, Septerna, Teva, ThirdHarmonic Bio, and Vifor. John Anderson is a speaker bureau member for CSL Behring, Pharming, BioCryst, Takeda, AstraZeneca, and GSK; has received consulting fees from CSL Behring, Pharming, BioCryst, Pharvaris, Ionis, Takeda, and Novartis; and is a clinical trial investigator for BioCryst, CSL Behring, Pharvaris, Kalvista, Biomarin, Astria, Takeda, Novartis, and Celldex. Neetu Talreja has been an investigator for 9Meters, AbbVie, Allakos, Amgen, Anaptybio Inc., Arena, ARS, AstraZeneca, Biohaven, Braintree, Celldex, Eli Lilly, Escient, GlaxoSmithKline, Gossamer, Incyte, Janssen, Knopp, Nerre, Novartis, Pearl Therapeutics, Pfizer, Phathom, Regeneron, Sanofi, Teva, and Upstream. She has also sat on advisory board(s) and been a medical consultant for Celldex, Novartis, and Regeneron. Jonathan A. Bernstein has been a PI, consultant, and speaker for Novartis, Genentech, AstraZeneca, Sanofi, Regeneron, BioCryst, CSL Behring, Takeda/Shire, Pharming, and GSK; PI and consultant for Celldex, Cogent, Escient, Jasper, Amgen, Roche, Ionis, Kalvista, Allakos, Biomarin, and Blueprint Medicine; PI for Allergy Therapeutics, Telios, Intellia, Aretrea, Pharvaris, Astria; PI for Teva; and consultant for Incyte, Astria, ONO, Cycle, Escient, Pharvaris, and TLL.
Figures
References
-
- Kolkhir P., Borzova E., Grattan C., Asero R., Pogorelov D., and Maurer M., “Autoimmune Comorbidity in Chronic Spontaneous Urticaria: A Systematic Review,” Autoimmunity Reviews 16 (2017): 1196–1208. - PubMed
-
- Zuberbier T., Abdul Latiff A. H., Abuzakouk M., et al., “The International EAACI/GA(2)LEN/EuroGuiDerm/APAAACI Guideline for the Definition, Classification, Diagnosis, and Management of Urticaria,” Allergy 77 (2022): 734–766. - PubMed
-
- Church M. K., Kolkhir P., Metz M., and Maurer M., “The Role and Relevance of Mast Cells in Urticaria,” Immunological Reviews 282 (2018): 232–247. - PubMed
-
- Elieh‐Ali‐Komi D., Metz M., Kolkhir P., et al., “Chronic Urticaria and the Pathogenic Role of Mast Cells,” Allergology International 72 (2023): 359–368. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
