

Left ventricular decompression in paediatric veno-arterial extracorporeal life support: Reviewing the evidence
- PMID: 40415596
- PMCID: PMC12287853
- DOI: 10.1002/ehf2.15325
Left ventricular decompression in paediatric veno-arterial extracorporeal life support: Reviewing the evidence
Abstract
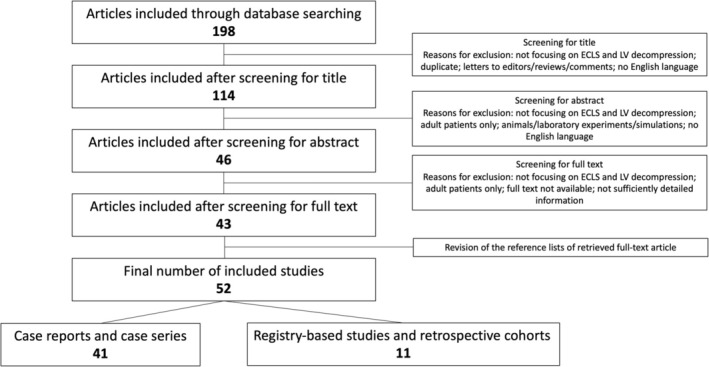
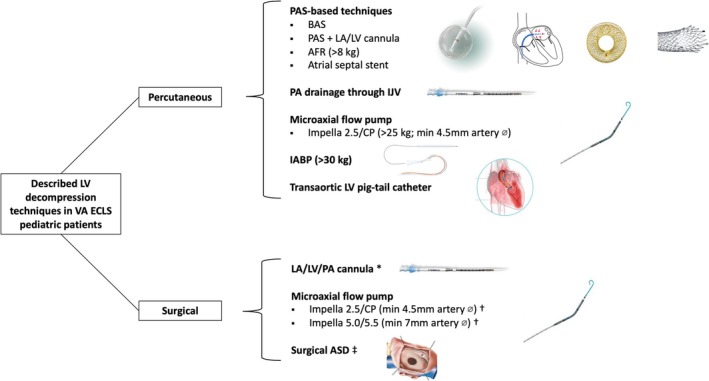
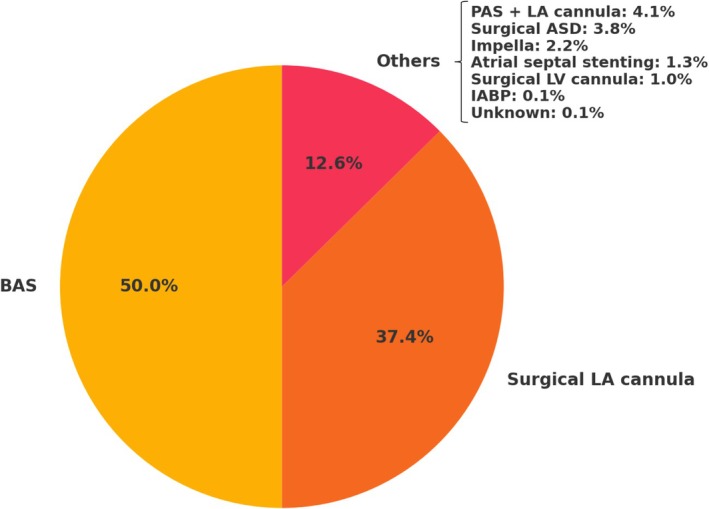
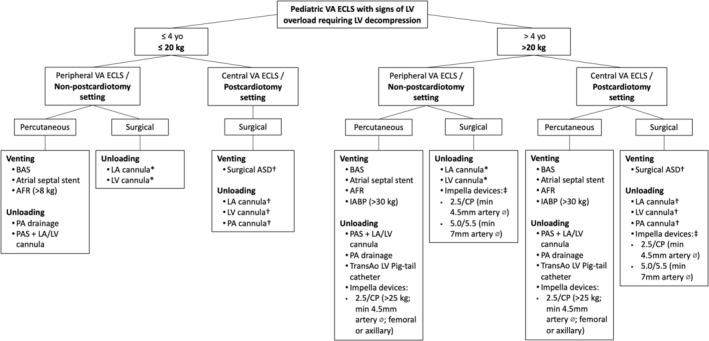
Veno-arterial extracorporeal life support (VA ECLS) is crucial for neonatal and paediatric patients with severe circulatory collapse but may cause left ventricular (LV) overload, affecting myocardial recovery and causing complications. Evidence on optimal LV decompression strategies in paediatric patients remains limited. We conducted a systematic review following PRISMA guidelines, including articles published between 1993 and 2024 focused on VA ECLS and LV decompression in patients under 18 years of age. The review included 11 retrospective cohorts and registry-based studies (2012-2024), totalling 1222 paediatric patients undergoing decompression. Patient demographics, initial diagnoses and VA ECLS settings were heterogeneous. The prevalence of LV decompression ranged from 46.6% in post-cardiotomy to 10.5% in non-post-cardiotomy peripheral VA ECLS cases. Most patients (57.1%) were supported with peripheral VA ECLS, and the majority (57.4%) underwent percutaneous decompression, whereas surgical approaches predominated in post-cardiotomy central VA ECLS. Balloon atrial septostomy (BAS) was the most frequent technique (50%), followed by surgically placed left atrial cannula (37.4%). Thirteen case series (70 patients) and 28 case reports (28 patients) were also reviewed. Substantial variability in LV decompression strategies exists based on age and clinical scenario. PAS-based techniques were more common in younger patients on peripheral VA ECLS while older children often underwent different strategies. Surgical approaches were preferred in central VA ECLS, particularly in the post-cardiotomy setting. Procedural safety varied by technique. While PAS-based strategies such as BAS generally showed low complication rates, adverse events like arrhythmia, bleeding and cardiac perforation were reported in 7%-9% of cases. Surgical LA cannulation was associated with higher bleeding risk. Impella use was linked to haemolysis (50%) and major bleeding (20%). Comparative data highlight that each technique carries distinct procedural risks and complication profiles. In conclusion, LV decompression during paediatric VA ECLS remains technically challenging and variably adopted. Its benefit appears more consistent in the post-cardiotomy setting, where improved survival and reduced adverse outcomes were observed. Given the lack of standardization, further prospective studies and collaborative registries are essential to guide strategy selection, timing and risk-benefit balance, particularly in such a vulnerable population.
Keywords: left ventricular decompression; paediatric; unloading; veno‐arterial extracorporeal life support; venting.
© 2025 The Author(s). ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Paolo Meani reports speaker honoraria from Xenios Fresenius Medical Care. Ravi R. Thiagarajan reports receiving speaker fees from the Society of Critical Care Medicine and funding from the US Department of Defense Clinical Trial Award (Trial of Indication‐based Transfusion of RBC in ECMO, #W81XWH2210301). Ryan P. Barbaro serves as a member of the Board of Directors for the Extracorporeal Life Support Organization and receives funding from the National Institutes of Health (R01 HL153519). Enrico Ammirati reports receiving a grant from the Italian Ministry of Health (GR‐2019‐12368506) as the principal investigator of the investigator‐driven MYTHS (Myocarditis Therapy with Steroids) trial; funding from the Italian Ministry of Health and NextGenerationEU (PNRR‐MAD‐2022‐12376225) and serves as a consultant for Lexeo, Kiniksa, AstraZeneca and Cytokinetics. Roberto Lorusso reports research grants from Medtronic and LivaNova paid to their institution; consulting fees from Medtronic and LivaNova paid to their institution; speaker honoraria from Abiomed; travel support from Medtronic and LivaNova; lab supplies from Medtronic, unrelated to the submitted work; and is an advisory board member for Eurosets and Xenios (fees paid to institution). Marc Dickstein reports speaker honoraria from Abiomed. The other authors report no conflicts of interest.
Figures
References
-
- Schrage B, Becher PM, Bernhardt A, Bezerra H, Blankenberg S, Brunner S, et al. Left ventricular unloading is associated with lower mortality in patients with cardiogenic shock treated with venoarterial extracorporeal membrane oxygenation: results from an international, multicenter cohort study. Circulation 2020;142:2095‐2106. doi: 10.1161/CIRCULATIONAHA.120.048792 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
