

Prognostic impact of biomarkers in PMBCL: rationale for early integration of immune checkpoint inhibitors
- PMID: 40416849
- PMCID: PMC12098338
- DOI: 10.37349/etat.2025.1002318
Prognostic impact of biomarkers in PMBCL: rationale for early integration of immune checkpoint inhibitors
Abstract
Aim: This research aims to guide future strategies for personalized treatment of primary mediastinal large B-cell lymphoma (PMBCL), particularly to identify high-risk patients who may benefit from incorporating immune checkpoint inhibitors (ICIs) in the first-line setting.
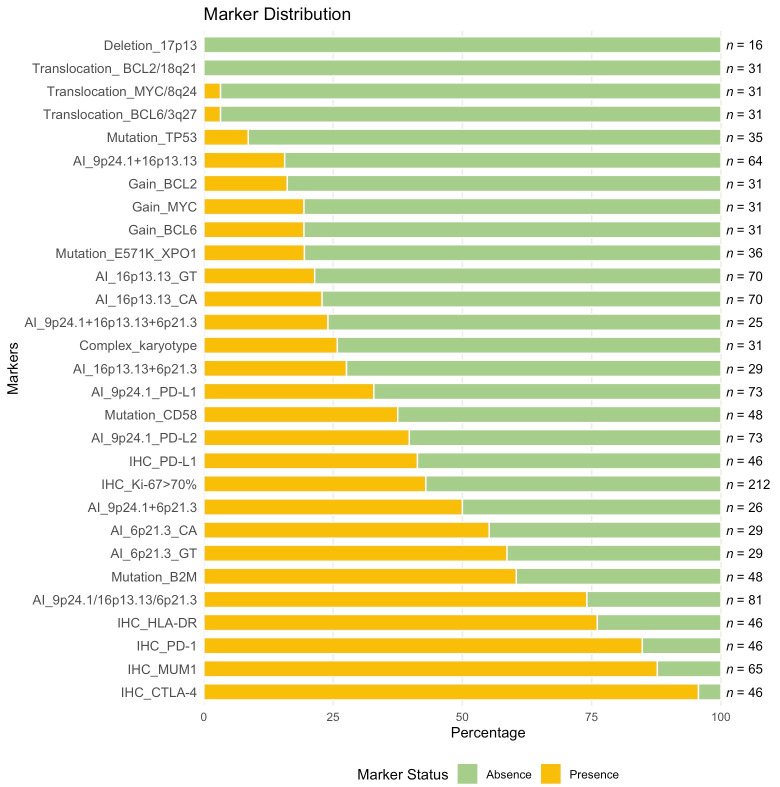
Methods: A retrospective, single-center study included 254 newly diagnosed PMBCL patients treated with rituximab, dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin (R-DA-EPOCH), rituximab, modified protocol NHL-BFM-90 (RmNHL-BFM-90), or R-DA-EPOCH combined with nivolumab. Clinical parameters, immunohistochemical markers [programmed death ligand-1 (PD-L1), programmed death-1 (PD-1), cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), human leucocyte antigen (HLA)-DR, Ki-67, multiple myeloma oncogene 1 (MUM1)], molecular markers (mutations in tumor protein p53 (TP53), CD58, beta-2-microglobulin (B2M), and exportin 1 (XPO1) genes; short tandem repeats at 6p21.3 [major histocompatibility complex (MHC) class I/II], 9p24.1 (PD-L1/PD-L2), 16p13.13 [class II, MHC, transactivator gene (CIITA)]), and cytogenetic profiles [myelocytomatosis oncogene (MYC)/8q24, B-cell lymphoma 2 (BCL2)/18q21, BCL6/3q27, del17p13, and karyotype abnormalities] were analyzed.
Results: The addition of nivolumab to R-DA-EPOCH as a first-line regimen significantly improved event-free survival (EFS; P = 0.018). This study identified that adverse prognostic factors for PMBCL include allelic imbalance at specific loci 6p21.3 (MHC class I/II), 9p24.1 (PD-L1/PD-L2), and 16p13.13 (CIITA). Incorporating nivolumab into the R-DA-EPOCH regimen as a first-line therapy has shown potential in reducing adverse prognostic factors.
Conclusions: These findings suggest that high-risk patients may benefit significantly from the early incorporation of ICIs into their treatment plans.
Keywords: PMBCL; genomic instability; immune checkpoint inhibitors; loss of heterozygosity.
© The Author(s) 2025.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures






References
-
- Camus V, Drieux F, Jardin F. State of the art in the diagnosis, biology and treatment of primary mediastinal B-cell lymphoma: a review. Ann Lymphoma. 2022;6:13. doi: 10.21037/aol-22-13. - DOI
-
- Cazals-Hatem D, Lepage E, Brice P, Ferrant A, d’Agay MF, Baumelou E, et al. Primary mediastinal large B-cell lymphoma. A clinicopathologic study of 141 cases compared with 916 nonmediastinal large B-cell lymphomas, a GELA (“Groupe d’Etude des Lymphomes de l’Adulte”) study. Am J Surg Pathol. 1996;20:877–88. doi: 10.1097/00000478-199607000-00012. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous