

[Management of collaterals after Glenn procedure and its impact on patients with a single ventricle: a single-center study]
- PMID: 40417334
- PMCID: PMC12097323
- DOI: 10.24875/RECIC.M24000475
[Management of collaterals after Glenn procedure and its impact on patients with a single ventricle: a single-center study]
Abstract
Introduction and objectives:: The bidirectional Glenn shunt (BDG) is an essential step in the repair of a physiologically single-ventricle heart. BDG increases pulmonary blood flow, allows growth of the pulmonary arteries, and improves SaO2. The procedure also allows unloading of ventricular volume, thereby improving survival. Our aim was to register all patients who developed collaterals following BDG, document the management methods used, and assess their impact.
Methods:: We included 56 patients who underwent BDG procedures at a median age of 2.08 (1-3) years. After BDG, peripheral pulmonary stenting was used in 2 patients. Symptomatic hyperviscosity was present in 10 patients (17.86%), who underwent venesection. BDG was unsuccessful in 2 patients. Venovenous collaterals were observed in 41 patients (73.2%), and aortopulmonary collaterals in 37 (66.1%).
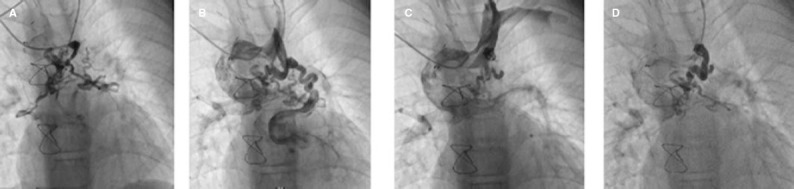
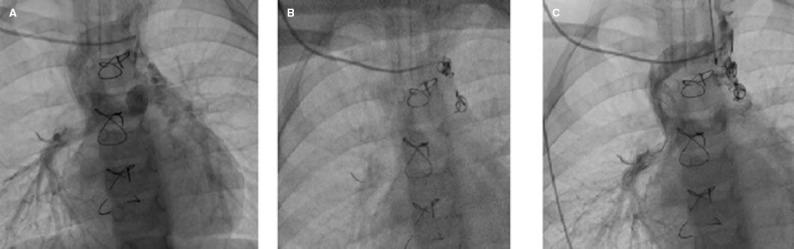
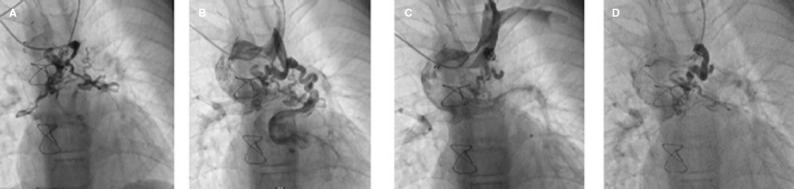
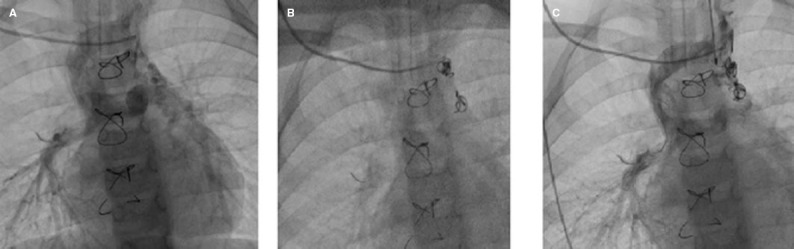
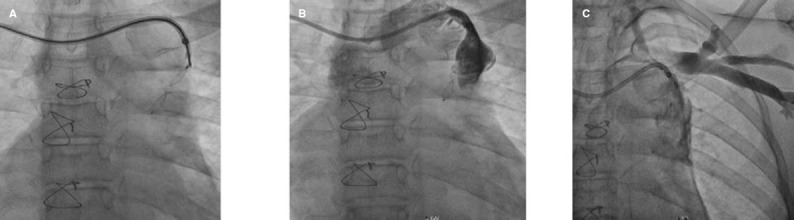
Results:: Hematocrit levels were significantly higher in patients with venovenous collaterals (50.00 ± 8.76) than in those without (P = .031). Mean pulmonary artery pressure was also significantly higher in patients with venovenous collaterals (15 [12-18] mmHg; P = .025). One patient had undergone successful closure of venovenous collaterals to epicardial veins and abdominal veins 3 years previously. Seven patients underwent transcatheter closure (TCC) of collaterals. Of these, 4 patients underwent TCC of venovenous collaterals to left and right pulmonary veins; 1 patient underwent closure of an aortopulmonary collateral; 1 patient underwent a failed attempt at venovenous collateral closure that was complicated by an ischemic stroke; and 1 patient had localized extravasation upon separation of the cable. A highly statistically significant increase in SaO2 was observed after TCC of venovenous collaterals (69.83 ± 10.91 vs 82.83 ± 9.87; P = .008).
Conclusions:: TCC of collaterals is a technically demanding but effective management strategy following BDG to improve patients’ SaO2 and quality of life. Awareness of possible complications and their effective management is crucial.
Keywords: Aortopulmonary collaterals; Coil embolization; Device embolization; Pulmonary vein; Transcatheter closure; Venovenous.
Copyright: © 2024 Sociedad Española de Cardiología.
Conflict of interest statement
CONFLICTO DE INTERESES: Ninguno.
Figures



References
-
- Liu S, Joseph KS, Lisonkova S, et al. Association between maternal chronic conditions and congenital heart defects:a population-based cohort study. Circulation. 2013;128:583-589. - PubMed
- Liu S, Joseph KS, Lisonkova S, et al. Association between maternal chronic conditions and congenital heart defects:a population-based cohort study. Circulation. 2013;128:583–589. - PubMed
-
- Mocumbi AO, Lameira E, Yaksh A, et al. Challenges on the management of congenital heart disease in developing countries. Int J Cardiol. 2011;148:285-288. - PubMed
- Mocumbi AO, Lameira E, Yaksh A, et al. Challenges on the management of congenital heart disease in developing countries. Int J Cardiol. 2011;148:285–288. - PubMed
-
- Salik I, Mehta B, Ambati S. Bidirectional Glenn procedure or hemi-Fontan [Internet], Treasure Island (FL):StatPearls Publishing;2022. Disponible en:https://www.ncbi.nlm.nih.gov/books/NBK563299/. Consultado 17 Jun 2024. - PubMed
- Salik I, Mehta B, Ambati S. Bidirectional Glenn procedure or hemi-Fontan [Internet] Treasure Island (FL): StatPearls Publishing; 2022. Disponible en: https://www.ncbi.nlm.nih.gov/books/NBK563299/ Consultado 17 Jun 2024. - PubMed
-
- Dilawar M, Gottliebson WM, Bradley SM, et al. Rapid development of a large systemic-to-pulmonary vein fistula after bidirectional Glenn shunt and successful closure with an Amplatzer duct occluder. Circulation. 2001;104:E41-E42. - PubMed
- Dilawar M, Gottliebson WM, Bradley SM, et al. Rapid development of a large systemic-to-pulmonary vein fistula after bidirectional Glenn shunt and successful closure with an Amplatzer duct occluder. Circulation. 2001;104:E41. - PubMed
Publication types
LinkOut - more resources
Full Text Sources