

Biotin interference in routine clinical immunoassays
- PMID: 40417451
- PMCID: PMC12099460
- DOI: 10.1016/j.plabm.2025.e00472
Biotin interference in routine clinical immunoassays
Abstract
Background: Laboratory examinations play a crucial role in medical diagnostics and treatment, necessitating the identification of interference factors to ensure accurate results. Biotin, a common dietary supplement, can interfere with immunoassays utilizing biotin-streptavidin interactions. Studies have documented biotin's significant impact on thyroid function tests and various immunoassays, prompting the need for effective mitigation strategies.
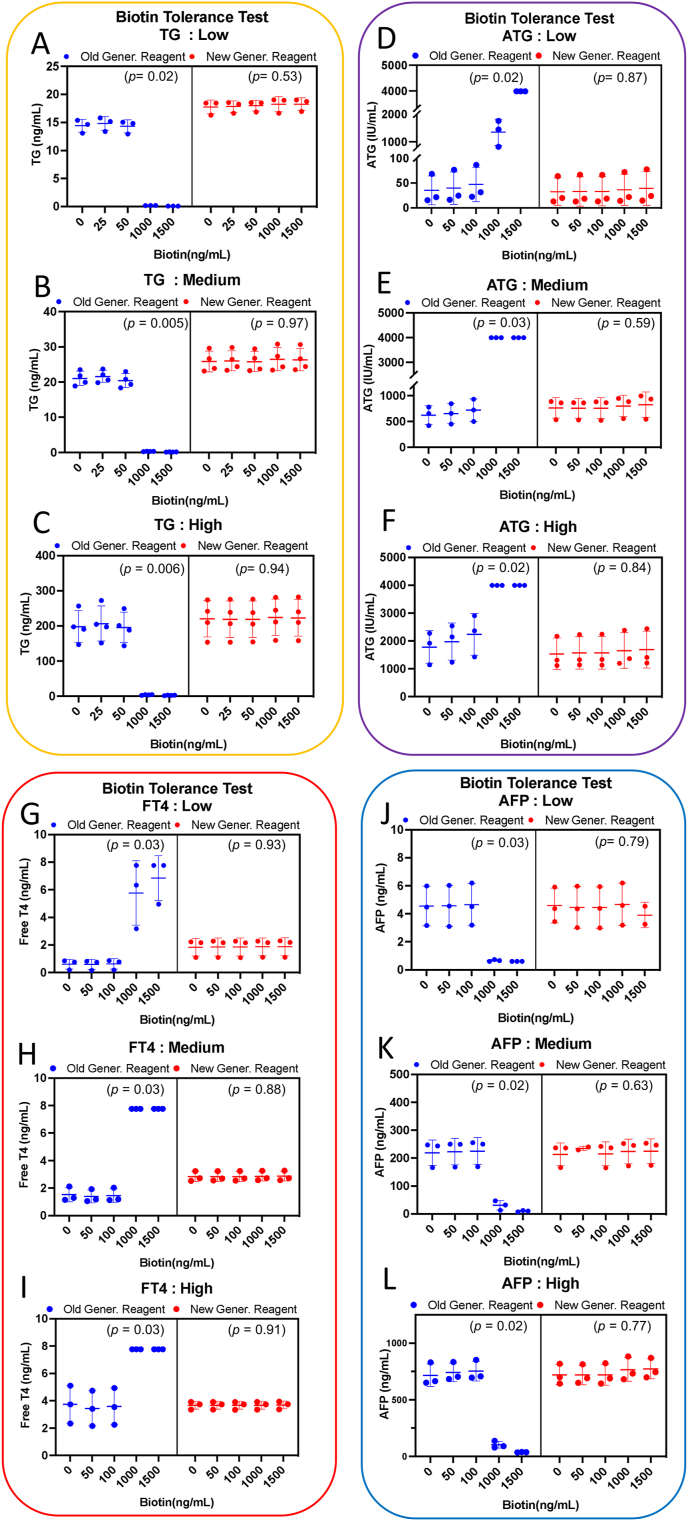
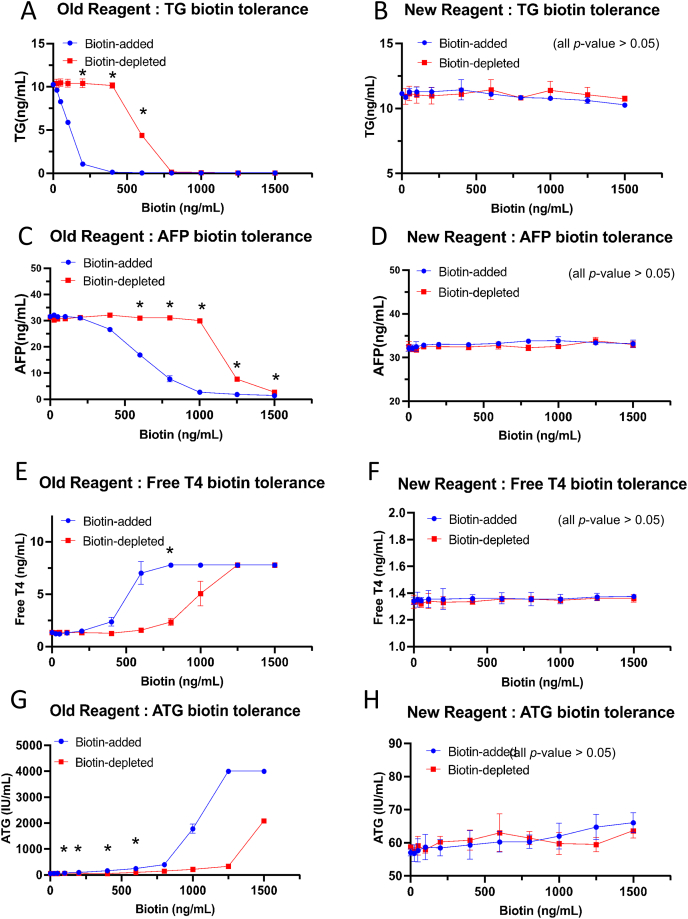
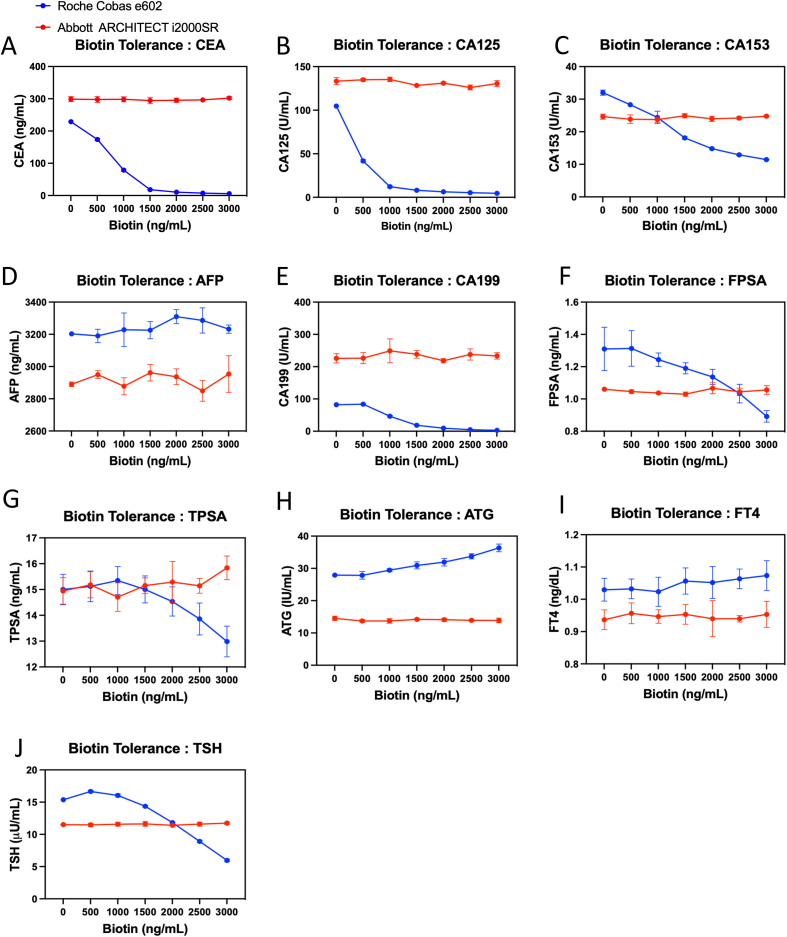
Methods: Samples were collected from various clinical departments and analyzed for biotin levels. Biotin interference was evaluated using both old and new Elecsys reagents in assays for thyroglobulin (TG), alpha-fetoprotein (AFP), anti-thyroglobulin (ATG), and free thyroxine (FT4). Biotin spike-in and depletion tests were conducted to assess interference mitigation methods. Additionally, the biotin tolerance of Roche and Abbott immunoassay systems was compared.
Results: Biotin levels were measured in 78 participants from different clinical departments: health management center (n = 13), emergency department (n = 21), intensive care unit (n = 12), gynecology department(n = 3), and hemodialysis department (n = 29). Patients undergoing hemodialysis and those in the intensive care unit (ICU) demonstrated significantly elevated biotin levels (mean = 3.282 ng/mL and 3.212 ng/mL, respectively) in comparison to other patient groups (p < 0.05), likely attributable to the intake of biotin-containing supplements. Biotin levels >500 ng/mL caused a 20 % change in assay values, resulting in false-low results for TG and AFP and false-high results for ATG and FT4 with older Elecsys reagents. Setting a 10 % change as the threshold, the newer Elecsys reagents demonstrated improved resistance against biotin interference, tolerating concentrations of 1000 ng/mL to 3000 ng/mL depending on the specific tests, consistent with the Roche package inserts. We employed a biotin depletion method that effectively restored assay accuracy for older reagents, generally resulting in less than a 10 % change when biotin levels were below 400 ng/mL. However, this depletion method was unnecessary with the newer reagents due to their increased biotin tolerance. Comparing the Roche and Abbott systems revealed significant differences in biotin tolerance. The Abbott system demonstrated greater resilience to biotin interference, while the Roche system showed biotin interference in assays for carcinoembryonic antigen, cancer antigen 125, cancer antigen 153, cancer antigen 19-9, with changes exceeding 30 % at 500 ng/mL of biotin.
Conclusions: Our study highlights the high prevalence of elevated biotin levels in hemodialysis and ICU patients, serving as a critical reference for clinical result interpretation. We confirm that Roche's newer reagents exhibit enhanced biotin tolerance, consistent with the manufacturer's claims, and demonstrate that biotin depletion effectively restores assay accuracy. These findings provide valuable methodological guidance for mitigating biotin interference in clinical immunoassays.
Keywords: Biotin depletion; Biotin tolerance; Elecsys; Hemodialysis; ICU; Immunoassay interference.
© 2025 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Trambas C., Lu Z., Yen T., Sikaris K. Characterization of the scope and magnitude of biotin interference in susceptible Roche Elecsys competitive and sandwich immunoassays. Ann. Clin. Biochem. 2018;55:205–215. doi: 10.1177/0004563217701777. http://www.ncbi.nlm.nih.gov/pubmed/28875734 - DOI - PubMed
-
- Colon P.J., Greene D.N. Biotin interference in clinical immunoassays. J. Appl. Lab. Med. 2018;2:941–951. doi: 10.1373/jalm.2017.024257. http://www.ncbi.nlm.nih.gov/pubmed/33636825 - DOI - PubMed
-
- Pacheco-Alvarez D., Solórzano-Vargas R.S., Del Río A.L. Biotin in metabolism and its relationship to human disease. Arch. Med. Res. 2002;33:439–447. doi: 10.1016/s0188-4409(02)00399-5. http://www.ncbi.nlm.nih.gov/pubmed/12459313 - DOI - PubMed
-
- Grimsey P., Frey N., Bendig G., Zitzler J., Lorenz O., Kasapic D., Zaugg C.E. Population pharmacokinetics of exogenous biotin and the relationship between biotin serum levels and in vitro immunoassay interference. Int. J. Pharmacokinet. 2017;2:247–256. doi: 10.4155/ipk-2017-0013. - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous
