

Investigation of the hyperperfusion phenomenon following carotid artery stenting using preoperative computed tomography perfusion imaging
- PMID: 40418407
- PMCID: PMC12106584
- DOI: 10.1007/s00701-025-06545-0
Investigation of the hyperperfusion phenomenon following carotid artery stenting using preoperative computed tomography perfusion imaging
Abstract
Purpose: This study aimed to identify the most effective parameters of computed tomography perfusion imaging (CTP) using the Bayesian estimation to predict hyperperfusion phenomenon (HPP) risk after carotid artery stenting (CAS).
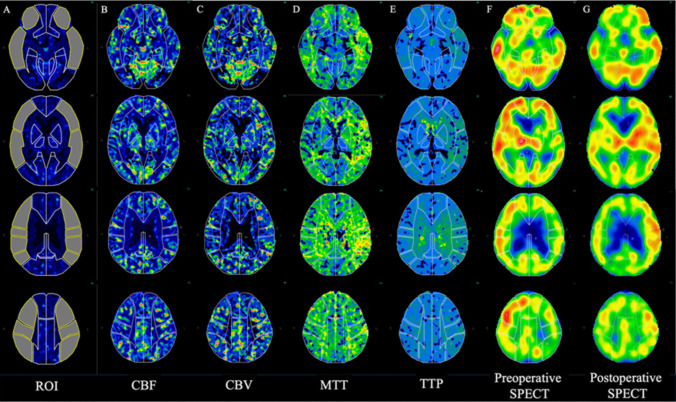
Methods: We retrospectively analyzed 46 patients who underwent CAS with preoperative CTP and preoperative and postoperative 123I-labeled N-isopropyl-p-iodoamphetamine (123I-IMP) single photon emission computed tomography (SPECT) at rest, between April 2019 and March 2024. Patients were categorized into the HPP and non-HPP groups based on the postoperative asymmetry index (AI) of cerebral blood flow (CBF) on 123I-IMP SPECT. Relative ratios of CBF, cerebral blood volume (CBV), mean transit time (MTT), and time-to-peak (TTP) were calculated from preoperative CTP and compared between the two groups. Correlations among each CTP parameter, preoperative AI, and postoperative AI were assessed. Receiver operating characteristic (ROC) analysis identified the most accurate CTP parameters for predicting HPP.
Results: HPP occurred in four patients, with one developing cerebral hemorrhage. Significant differences were observed between the HPP and non-HPP groups in CBV (p = 0.001), MTT (p = 0.003), and TTP ratio (p = 0.011), and preoperative AI (p = 0.021). Among the CTP parameters and preoperative AI, the CBV ratio showed a positive correlation with the postoperative AI (r = 0.63, p < 0.01). The CBV ratio demonstrated the highest area under the curve (AUC) for predicting HPP (AUC = 0.95). However, after Benjamini-Hochberg correction, statistical significance was lost (adjusted p = 0.07).
Conclusion: This study evaluated the predictive value of preoperative CTP using the Bayesian estimation method for identifying HPP risk after CAS. CBV ratio may serve as a potential parameter for predicting HPP.
Keywords: Carotid artery stenting; Computed tomography perfusion imaging; Hyperperfusion phenomenon; Hyperperfusion syndrome; Single photon emission computed topography.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: All procedures involving human participants performed in this study were in accordance with the ethical standards of the institutional committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Ethics Committee of Kyoto Prefectural University of Medicine Hospital (Approval No: ERB-C- 2730). In conducting this research, we strictly adhered to the Personal Information Protection Law regarding the handling of personal information of the participants based on the Declarations of Helsinki. Informed consent: Informed consent for participation was obtained through an opt-out process due to the anonymity of data, as approved by the ethics committee. Consent to publish: The authors declare their consent for publication. Competing interests: The authors declare no competing interests.
Figures



References
-
- Abbott AL (2009) Medical (nonsurgical) intervention alone is now best for prevention of stroke associated with asymptomatic severe carotid stenosis: results of a systematic review and analysis. Stroke 40:e573–e583. 10.1161/STROKEAHA.109.556068 - PubMed
-
- Buczek J, Karliński M, Kobayashi A, Białek P, Członkowska A (2013) Hyperperfusion syndrome after carotid endarterectomy and carotid stenting. Cerebrovascular Dis 35:531–537. 10.1159/000350736 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
