

Effectiveness of Digital Health Interventions for Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-Analysis
- PMID: 40418567
- PMCID: PMC12149779
- DOI: 10.2196/76323
Effectiveness of Digital Health Interventions for Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-Analysis
Abstract
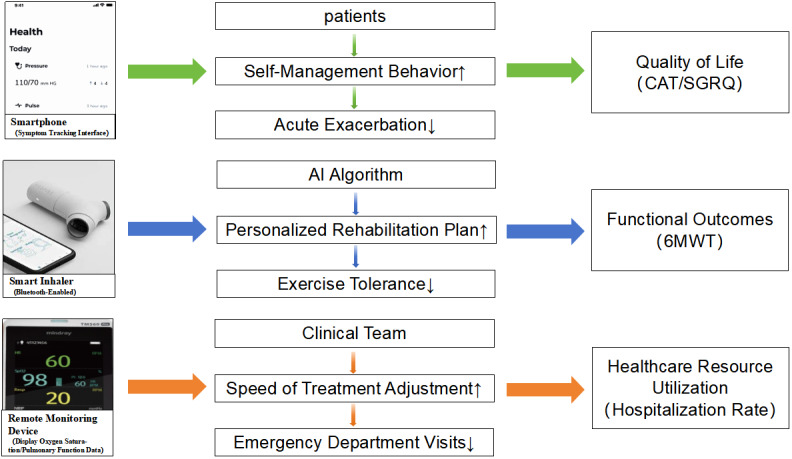
Background: Chronic obstructive pulmonary disease (COPD), marked by dyspnea, cough, and sputum production, significantly impairs patients' quality of life and functionality. Effective management strategies, particularly those empowering patients to manage their condition, are essential to reduce this burden and health care use. Digital health interventions-such as mobile apps for symptom tracking, wearable sensors for vital sign monitoring, and web-based pulmonary rehabilitation programs-can enhance self-efficacy and promote greater patient engagement. By improving self-management skills, these interventions also help alleviate pressure on health care systems.
Objective: This systematic review and meta-analysis assesses the clinical effectiveness of smartphone apps, wearable monitors, and web-delivered platforms in four COPD management areas: (1) quality of life (measured by the COPD Assessment Test [CAT] and St George's Respiratory Questionnaire), (2) self-efficacy (assessed by the General Self-Efficacy Scale), (3) functional capacity (evaluated via the 6-minute walk test and Modified Medical Research Council Dyspnea Scale), and (4) health care use (indicated by hospital and emergency department visits).
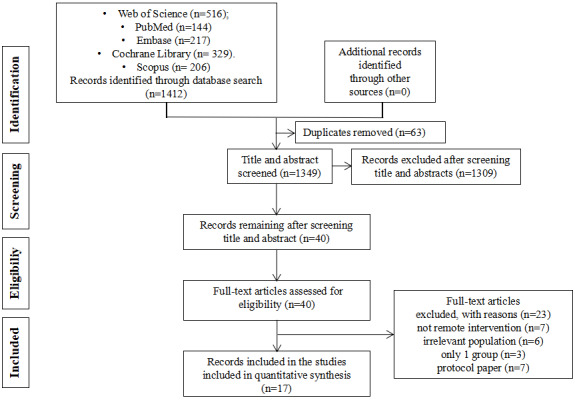
Methods: A systematic review was conducted using predefined search terms in PubMed, Embase, Cochrane, and Web of Science up to January 26, 2025, to identify randomized trials on digital health interventions for COPD. Two reviewers independently screened studies and extracted data. Outcomes included quality of life, self-efficacy, functional status, and health care use.
Results: This review included 17 studies with 2027 participants from 11 countries. Eleven trials involved health care professionals in digital platform use, and 12 reported adherence strategies. Digital tools for COPD primarily focused on telerehabilitation (eg, video-guided exercises) and self-management systems (eg, artificial intelligence-driven exacerbation alerts). The study participants were predominantly older adults. Meta-analysis results indicated that digital health interventions significantly improved quality of life at 3 months on the CAT (mean difference [MD] -1.65, 95% CI -3.17 to -0.14; P=.03); at 6 months on the CAT (MD -2.43, 95% CI -3.93 to -0.94; P=.001) and St George's Respiratory Questionnaire (MD 3.25, 95% CI 0.69-5.81; P=.01); at 12 months on the CAT (MD -2.53, 95% CI -3.91 to -1.16; P<.001), EQ-5D (MD 0.04, 95% CI 0.01-0.07; P=.02), and EQ-5D visual analogue scale (MD 5.88, 95% CI 0.38-11.37; P=.04); the General Self-Efficacy Scale at 3 months (MD 1.65, 95% CI 0.62-2.69; P=.002) and 6 months (MD 1.94, 95% CI 0.83-3.05; P<.001); and the Modified Medical Research Council Dyspnea Scale at more than 3 months (MD -0.23, 95% CI -0.36 to -0.11; P=.003). However, no significant differences were observed in the 6-minute walk test, emergency department admissions, hospital admissions, emergency department admissions for COPD, or hospital admissions for COPD.
Conclusions: Our findings suggest that digital health interventions may benefit COPD patients, but their clinical effectiveness remains uncertain. Further robust studies are needed, particularly those involving larger numbers of older adults with COPD.
Trial registration: PROSPERO CRD420251032053; https://www.crd.york.ac.uk/PROSPERO/view/CRD420251032053.
Keywords: chronic respiratory disease; evidence synthesis; mHealth; mobile health; remote patient monitoring; self-management; telemedicine.
©Miaoqing Zhuang, Intan Idiana Hassan, Wan Muhamad Amir W Ahmad, Azidah Abdul Kadir, Xiaodong Liu, Furong Li, Yinuo Gao, Yang Guan, Shuting Song. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 26.05.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures























References
-
- GBD 2016 Occupational Chronic Respiratory Risk Factors Collaborators Global and regional burden of chronic respiratory disease in 2016 arising from non-infectious airborne occupational exposures: a systematic analysis for the Global Burden of Disease Study 2016. Occup Environ Med. 2020 Mar;77(3):142–150. doi: 10.1136/oemed-2019-106013. http://oem.bmj.com/lookup/pmidlookup?view=long&pmid=32054818 oemed-2019-106013 - DOI - PMC - PubMed
-
- Prasad B. Chronic obstructive pulmonary disease (COPD) Int J Pharm Res Technol. 2020;10(1):67–71. doi: 10.31838/ijprt/10.01.12. - DOI
-
- Zhong N, Wang C, Yao W, Chen P, Kang J, Huang S, Chen B, Wang C, Ni D, Zhou Y, Liu S, Wang X, Wang D, Lu J, Zheng J, Ran P. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey. Am J Respir Crit Care Med. 2007 Oct 15;176(8):753–60. doi: 10.1164/rccm.200612-1749OC.200612-1749OC - DOI - PubMed
-
- Zhou M, Wang H, Zeng X, Yin P, Zhu J, Chen W, Li X, Wang L, Wang L, Liu Y, Liu J, Zhang M, Qi J, Yu S, Afshin A, Gakidou E, Glenn S, Krish VS, Miller-Petrie MK, Mountjoy-Venning WC, Mullany EC, Redford SB, Liu H, Naghavi M, Hay SI, Wang L, Murray CJ, Liang X. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019 Sep 28;394(10204):1145–58. doi: 10.1016/S0140-6736(19)30427-1. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(19)30427-1 S0140-6736(19)30427-1 - DOI - PMC - PubMed
-
- Guarascio AJ, Ray SM, Finch CK, Self TH. The clinical and economic burden of chronic obstructive pulmonary disease in the USA. Clinicoecon Outcomes Res. 2013;5:235–45. doi: 10.2147/CEOR.S34321. https://www.tandfonline.com/doi/abs/10.2147/CEOR.S34321?url_ver=Z39.88-2... ceor-5-235 - DOI - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
