

Unilateral biportal endoscopic versus microscopic discectomy in degenerative lumbar spinal stenosis: A prospective cohort study
- PMID: 40419907
- PMCID: PMC12113972
- DOI: 10.1097/MD.0000000000042594
Unilateral biportal endoscopic versus microscopic discectomy in degenerative lumbar spinal stenosis: A prospective cohort study
Abstract
Background: Unilateral biportal endoscopic discectomy (UBE) and microendoscopic discectomy (MED) are well-established minimally invasive techniques for managing single-segment degenerative lumbar spinal stenosis (DLSS). However, current evidence from evidence-based medicine remains insufficient to conclusively demonstrate the comparative advantages of these methods.
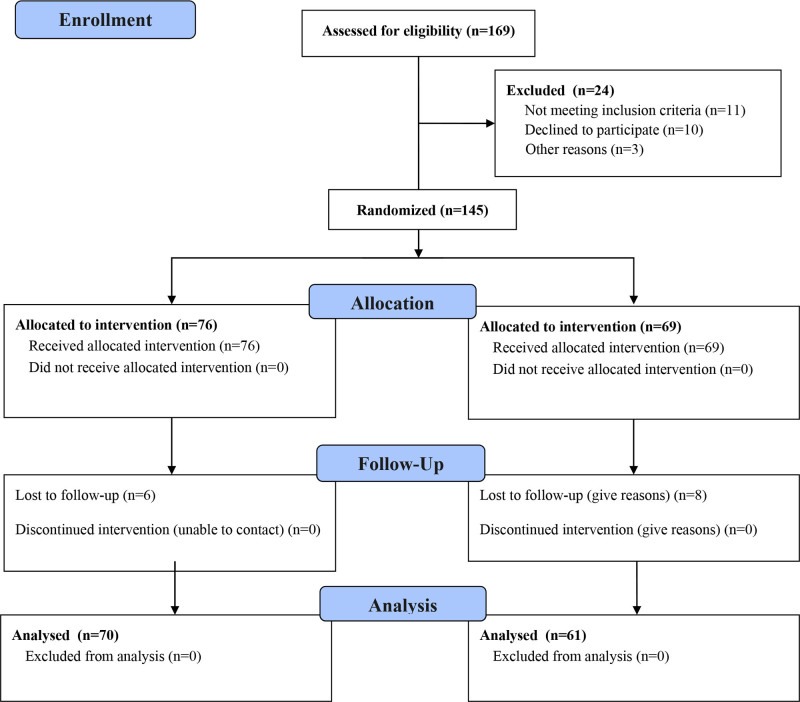
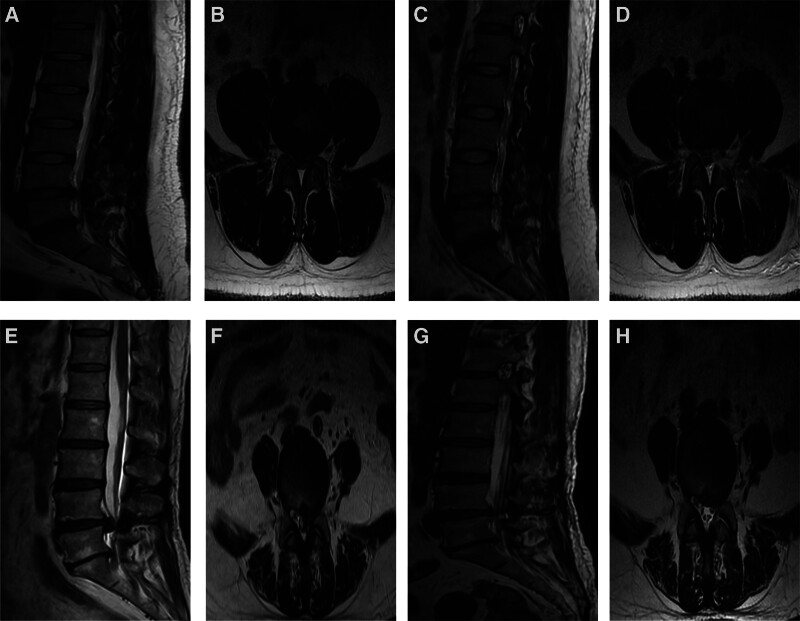
Methods: A total of 145 patients diagnosed with single-segment DLSS were enrolled from the spinal surgery department of Xinjiang Bazhou People's Hospital between January 2022 and August 2024. Fourteen patients were lost to follow-up, leaving 131 valid cases. Participants were divided into 2 groups: UBE (n = 70) and MED (n = 61), based on the surgical approach. The study compared the demographic and clinical characteristics of both groups (gender, age, disease duration, height, weight, BMI, and affected segment), perioperative metrics (operation time, blood loss, and hospital stay), and clinical outcomes at various time points (preoperatively, 3 days postoperatively, 1-month postoperatively, 3 months postoperatively, 1-year postoperatively, and 2 years postoperatively), including visual analogue scale (VAS) scores for back and leg pain, Oswestry disability index (ODI) scores, and imaging parameters (preoperative and postoperative disc height and dural sac expansion area).
Results: All patients completed follow-up for over 2 years. The UBE group demonstrated significantly shorter operation times, reduced blood loss, and shorter hospital stays compared to the MED group (P < .05). No significant differences in VAS scores for back and leg pain or ODI scores were found between the groups at preoperative and postoperative time points (P > .05). Both groups showed significant improvements in VAS scores for back and leg pain and ODI scores at all postoperative time points relative to preoperative levels (P < .05). No significant differences in dural sac expansion area or disc height (preoperative and postoperative) were noted between the groups (P > .05).
Conclusion: Both UBE and MED are effective treatments for single-segment DLSS, achieving substantial spinal canal decompression and improvement in clinical symptoms. UBE, however, offers advantages over MED in terms of shorter surgical time, reduced blood loss, and shorter hospital stays.
Keywords: MED; UBE; degenerative lumbar spinal stenosis; microendoscopic discectomy; unilateral biportal endoscopic.
Copyright © 2025 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Webb CW, Aguirre K, Seidenberg PH. Lumbar spinal stenosis: diagnosis and management. Am Fam Physician. 2024;109:350–9. - PubMed
-
- Katz JN, Zimmerman ZE, Mass H, Makhni MC. Diagnosis and management of lumbar spinal stenosis: a review. JAMA. 2022;327:1688–99. - PubMed
-
- Schönnagel L, Zhu J, Camino-Willhuber G, et al. Relationship between lumbar spinal stenosis and axial muscle wasting. Spine J. 2024;24:231–8. - PubMed
-
- Feng Z, Zhao Z, Cui W, Meng X, Hai Y. Unilateral biportal endoscopic discectomy versus microdiscectomy for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2024;33:2139–53. - PubMed
-
- He J, Xiao S, Wu Z, Yuan Z. Microendoscopic discectomy versus open discectomy for lumbar disc herniation: a meta-analysis. Eur Spine J. 2016;25:1373–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
