

Clinical characteristics of headache related to epilepsy: experience from a tertiary epilepsy center
- PMID: 40420007
- PMCID: PMC12105137
- DOI: 10.1186/s12883-025-04217-1
Clinical characteristics of headache related to epilepsy: experience from a tertiary epilepsy center
Abstract
Background: Headache is one of the most common diseases in epilepsy, with affected patients experiencing various types of headaches. This study aimed to investigate differences in headache types across epilepsy types, comparing pain levels among epilepsy patients with multiple headache types, and exploring associations between headache characteristics and epilepsy prognosis.
Methods: We retrospectively analyzed consecutive adult epilepsy patients with headache, collecting comprehensive sociodemographic, epilepsy-related, and headache-related data, as well as data on headache-attributed lost time and quality of life. The overall prevalence of headache in epilepsy patients was determined, and we compared clinical characteristics, quality of life, and headache-attributed lost time across different epilepsy types. Based on the temporal relationship between headache and seizures, headache related to epilepsy were classified into inter-ictal headache (Inter-IH), ictal headache, pre-ictal headache (Pre-IH), and post-ictal headache (Post-IH) for subgroup analysis to explore differences in clinical characteristics by headache type. We conducted multiple logistic regression and receiver operating characteristic (ROC) analyses to calculate the area under the curve (AUC), assessing correlations between headache characteristics and epilepsy prognosis and the predictive accuracy for drug-resistant epilepsy (DRE).
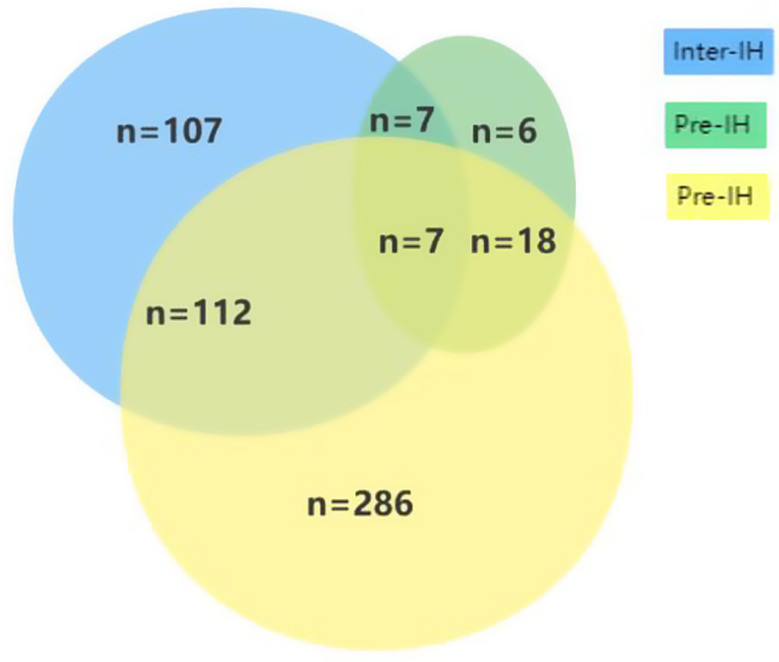
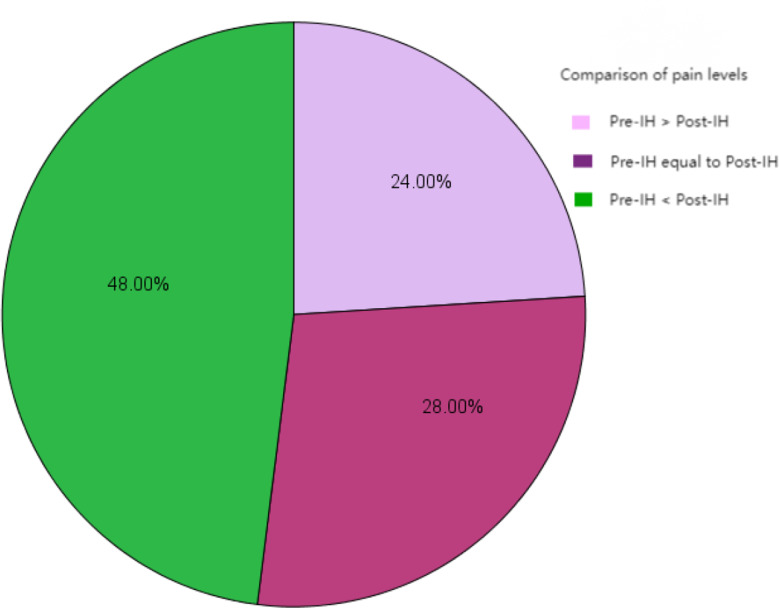
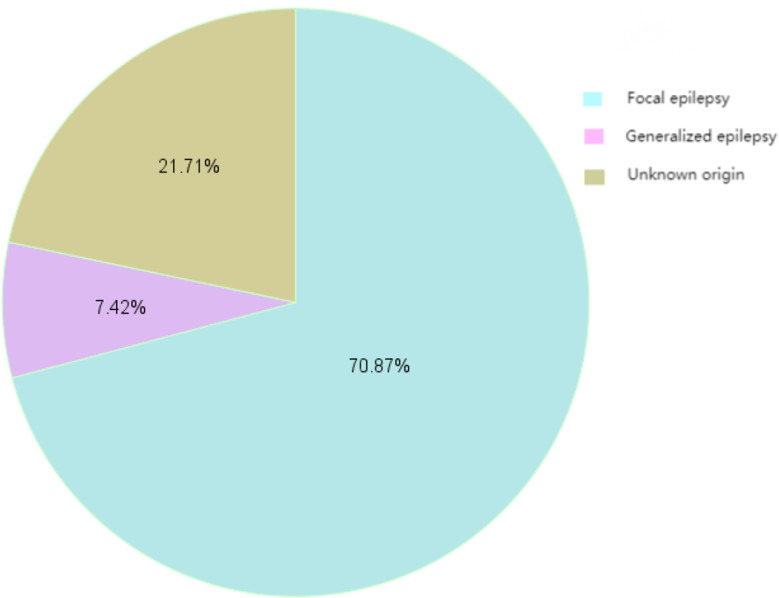
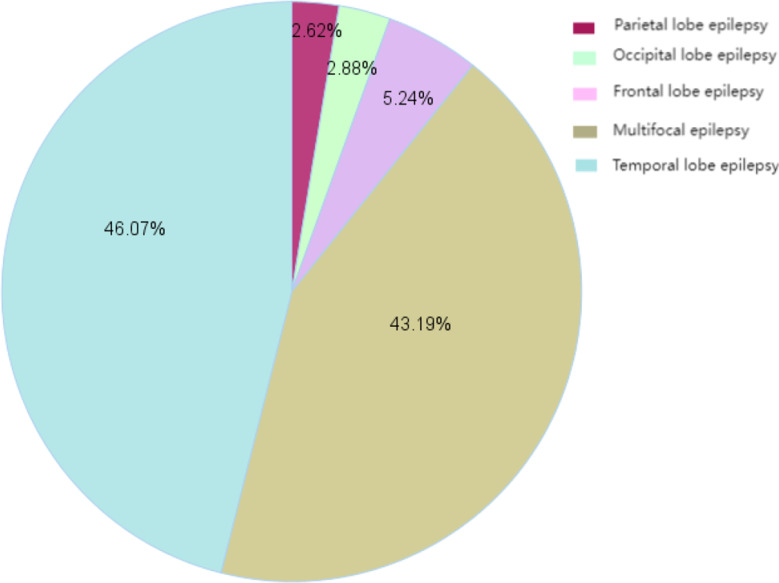
Results: A total of 539 epilepsy patients were included, comprising 233 with Inter-IH (43.22%), 38 with Pre-IH (7.05%), and 423 with Post-IH (78.48%); no patients had ictal headache. Among those with Inter-IH, 58 (10.76%) met the diagnostic criteria for migraine, and 87 (16.14%) met the criteria for tension-type headache. In our cohort, 7 patients (1.30%) experienced both Inter-IH and Pre-IH, 112 (22.08%) had both Inter-IH and Post-IH, 7 (1.30%) experienced Inter-IH, Pre-IH, and Post-IH, and 18 (3.34%) had both Pre-IH and Post-IH. The study included 382 patients with focal epilepsy (70.87%), 40 with generalized epilepsy (7.42%), and 117 with epilepsy of unknown origin (21.71%), with temporal lobe epilepsy being the most common focal type, representing 46.07% of cases. Patients with focal epilepsy reported lower quality of life than those with epilepsy of unknown origin (QOLIE-10, p < 0.05) and had a lower proportion of bilateral Post-IH than those with epilepsy of unknown origin (p < 0.05). The proportion of patients with level 1 Headache-Attributed Lost Time-90 Days (HALT-90) was higher in generalized epilepsy than in focal (87.50% vs. 66.23%, p < 0.05) and unknown origin (87.50% vs. 64.96%, p < 0.05). With migraine and HALT-90 were associated with DRE (p < 0.05), although predictive accuracy was low (AUC = 0.539; AUC = 0.566, respectively).
Conclusion: The most common type of epilepsy with headache was focal epilepsy, with patients experiencing poorer quality of life than those with epilepsy of unknown origin. Clinical characteristics of headache related epilepsy did not vary significantly by epilepsy type, but patients of generalized epilepsy with headache had the least time lost. Post-IH was the most common type of headache in epilepsy patients. With migraine and HALT-90 were associated with DRE, but the predictive accuracy for DRE was insufficient.
Keywords: Epilepsy type; Headache; Inter-ictal headache; Post-ictal headache; Pre-ictal headache.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The protocol conformed to the principles of the declaration of Helsinki and was approved by the institutional review board of West China Hospital of Sichuan University with the reference number 2022301. Written informed consent was obtained from all patients. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
A comparison of comorbid headache between patients with temporal lobe epilepsy and juvenile myoclonic epilepsy.Sci Rep. 2023 Oct 8;13(1):16962. doi: 10.1038/s41598-023-43705-7. Sci Rep. 2023. PMID: 37806981 Free PMC article.
-
Headache in epilepsy: prevalence and clinical features.J Headache Pain. 2015;16:556. doi: 10.1186/s10194-015-0556-y. Epub 2015 Aug 6. J Headache Pain. 2015. PMID: 26245188 Free PMC article.
-
The burden of headache in people with epilepsy.Seizure. 2016 Oct;41:120-6. doi: 10.1016/j.seizure.2016.07.018. Epub 2016 Aug 5. Seizure. 2016. PMID: 27543963
-
The complex interrelations between two paroxysmal disorders: headache and epilepsy.Neurol Sci. 2017 Jun;38(6):941-948. doi: 10.1007/s10072-017-2926-5. Epub 2017 Mar 24. Neurol Sci. 2017. PMID: 28341968 Review.
-
Links between headaches and epilepsy: current knowledge and terminology.Neurologia. 2014 Oct;29(8):453-63. doi: 10.1016/j.nrl.2011.10.016. Epub 2012 Jan 2. Neurologia. 2014. PMID: 22217520 Review. English, Spanish.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
