

Development and validation of a nomogram for predicting acute kidney injury risks in patients undergoing acute stanford type A aortic dissection repair surgery
- PMID: 40420010
- PMCID: PMC12105399
- DOI: 10.1186/s12882-025-04150-y
Development and validation of a nomogram for predicting acute kidney injury risks in patients undergoing acute stanford type A aortic dissection repair surgery
Abstract
Background: This study aims to construct and internally validate a comprehensive nomogram designed for accurately predicting the incidence of acute kidney injury (AKI) in patients undergoing repair surgery for acute Stanford Type A aortic dissection (ATAAD), thereby enhancing postoperative risk management and patient care strategies.
Methods: A retrospective analysis of 1471 consecutive patients diagnosed with ATAAD through computed tomography angiography (CTA) and confirmed by surgery at four tertiary medical centers from February 2010 to July 2023 was conducted. The study involved a comprehensive evaluation of 36 variables, categorizing patients into non-AKI and AKI groups. Advanced statistical techniques, including LASSO regression and Logistic regression, were employed. A sophisticated nomogram prediction model was developed using R language, and its efficacy was assessed using the concordance index (C-index), area under the receiver operating characteristic curve (AUC-ROC), and decision curve analysis.
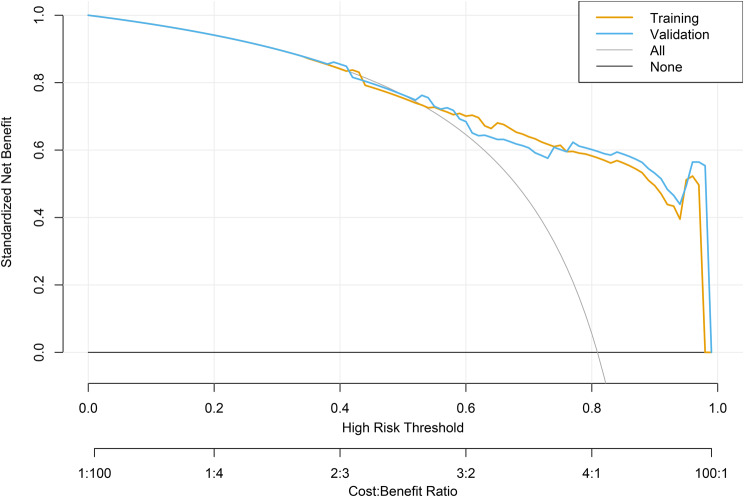
Results: Seven key factors independently predicting AKI were identified, including heart failure (a condition where the heart can't pump blood as well), hyperlipidemia (high levels of fats in the blood), arterial dissection (a serious condition where there is a tear in the wall of a blood vessel), renal insufficiency, blood urea nitrogen (BUN), abnormal electrocardiogram (ECG), and total cholesterol (TC). The AUC-ROC, a measure of the model's ability to distinguish between classes, was 0.850 (95% CI: 0.823-0.877) for the training set, with high sensitivity (76%) and specificity (99%). For the validation set, the AUC-ROC was 0.840 (95% CI: 0.798-0.833), with sensitivity and specificity of 78% and 94%, respectively. The nomogram demonstrated a recalibrated C-index of 0.854 for the training set and 0.752 for the validation set. Decision curve analysis revealed the nomogram's significant net benefit across various clinical threshold probabilities.
Conclusion: The AKI nomogram exhibits robust predictive capabilities, establishing itself as a crucial clinical tool for the early identification of patients at risk for AKI following ATAAD repair surgery. By delivering personalized risk assessments, this nomogram not only optimizes postoperative management strategies but also plays a vital role in enhancing patient outcomes through timely and proactive interventions.
Keywords: Acute kidney injury; Acute stanford type A aortic dissection; Nomogram; Predictive model; Retrospective analysis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All methods were carried out according to the relevant guidelines and regulations of the institutional and/or national research committee and the 1964 Helsinki Declaration. This study was approved by the Medical Ethics Committee (The First Hospital of Hebei Medical University, No. 7741-29), and informed consent was waived by the Medical Ethics Committee of The First Hospital of Hebei Medical University. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures





Similar articles
-
Risk prediction and prognostic analysis of post-implantation syndrome after thoracic endovascular aortic repair.Sci Rep. 2024 Jul 29;14(1):17376. doi: 10.1038/s41598-024-65877-6. Sci Rep. 2024. PMID: 39075074 Free PMC article.
-
Development and validation of a risk nomogram for postoperative acute kidney injury in older patients undergoing liver resection: a pilot study.BMC Anesthesiol. 2022 Jan 13;22(1):22. doi: 10.1186/s12871-022-01566-z. BMC Anesthesiol. 2022. PMID: 35026992 Free PMC article.
-
Development of a predictive nomogram for postoperative acute respiratory distress syndrome in Stanford type A aortic dissection patients: A retrospective study.Rev Port Cardiol. 2025 May;44(5):257-266. doi: 10.1016/j.repc.2024.10.006. Epub 2025 Jan 25. Rev Port Cardiol. 2025. PMID: 39870305 English, Portuguese.
-
[Development and validation of a nomogram for predicting 3-month mortality risk in patients with sepsis-associated acute kidney injury].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 May;36(5):465-470. doi: 10.3760/cma.j.cn121430-20231218-01091. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38845491 Chinese.
-
Prediction of Acute Kidney Injury for Acute Type A Aortic Dissection Patients Who Underwent Sun's Procedure by a Perioperative Nomogram.Cardiorenal Med. 2022;12(3):117-130. doi: 10.1159/000524907. Epub 2022 Jun 22. Cardiorenal Med. 2022. PMID: 35732144
References
-
- Wu YH, Jiang R, Li ZF, Pan YZ, Yang LS, Wang T, et al. Application of a modified extracorporeal circulation perfusion method during surgery for acute stanford type A aortic dissection. Heart Lung Circ. 2020;29:1203–09. - PubMed
-
- Roh GU, Lee JW, Nam SB, Lee J, Choi JR, Shim YH. Incidence and risk factors of acute kidney injury after thoracic aortic surgery for acute dissection. Ann Thorac Surg. 2012;94:766–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
