

Optimal parameters and Biomechanical analysis of the lightbulb technique for osteonecrosis of the femoral head: a finite element analysis
- PMID: 40420068
- PMCID: PMC12105154
- DOI: 10.1186/s12891-025-08763-0
Optimal parameters and Biomechanical analysis of the lightbulb technique for osteonecrosis of the femoral head: a finite element analysis
Abstract
Background: The lightbulb technique (LBT) is a common surgical procedure for treating peri-collapse osteonecrosis of the femoral head (ONFH). However, the drilling parameters and biomechanics of the technique have not been analyzed. The aim of this study was to optimize the biomechanical stability of the LBT by finite element (FE) analysis to guide intraoperative and postoperative schemes.
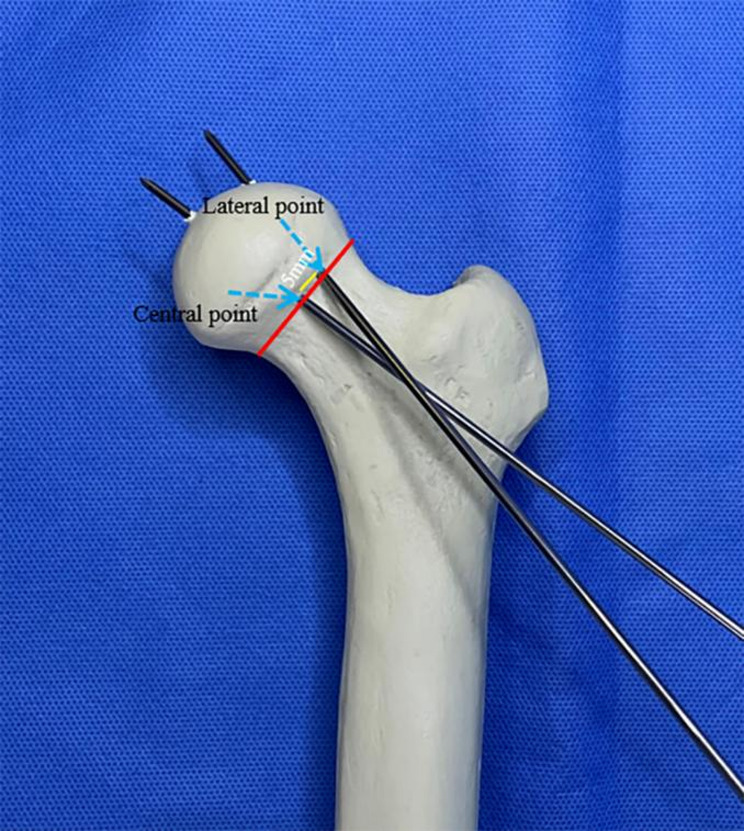
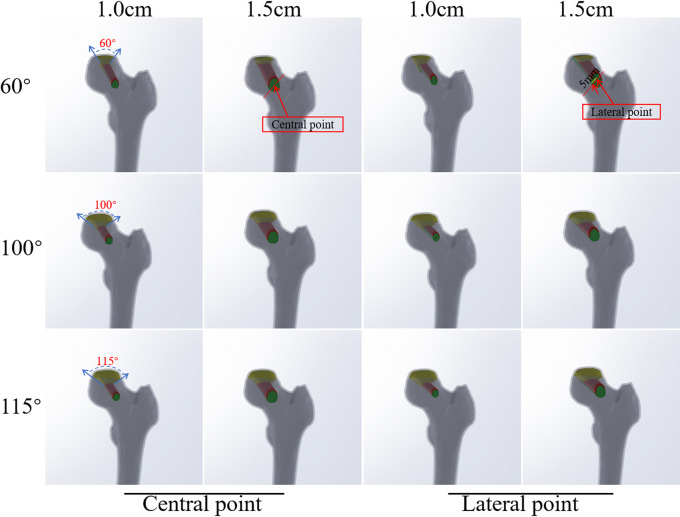
Methods: FE models were established based on computed tomography images of a healthy adult, including three different degrees of necrotic lesion (60°, 100°, 115°), drilling locations (points C and L) and diameters (1.0 cm, 1.5 cm). The stress of the drilling entrance area, superior and inferior edges of the femoral neck, and bone flap was evaluated under three different loads at 0.5 times body weight (0.5 BW, standing on two feet), 2.75 BW (standing on one foot), and 4 BW (walking with the middle foot on the ground).
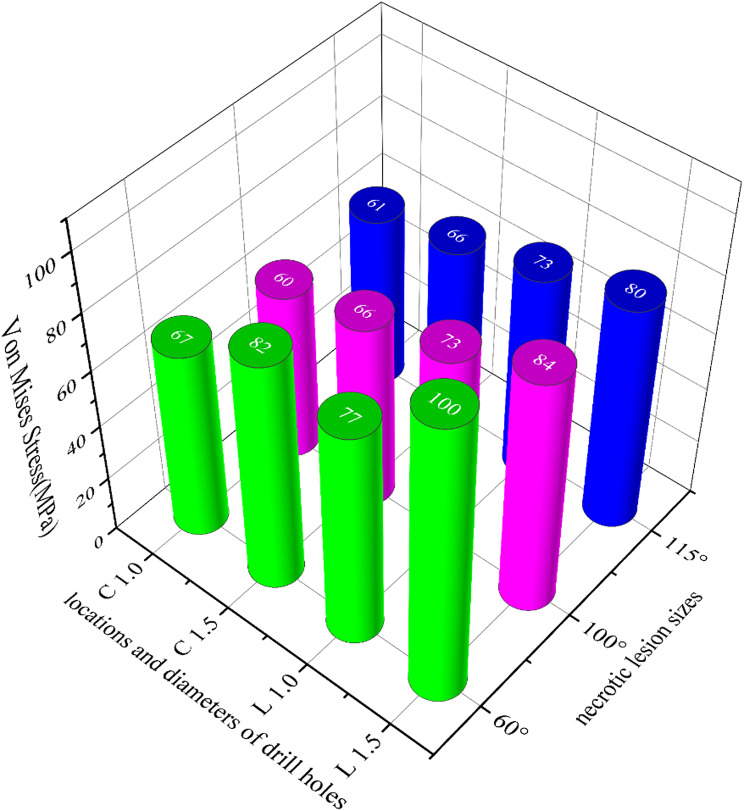
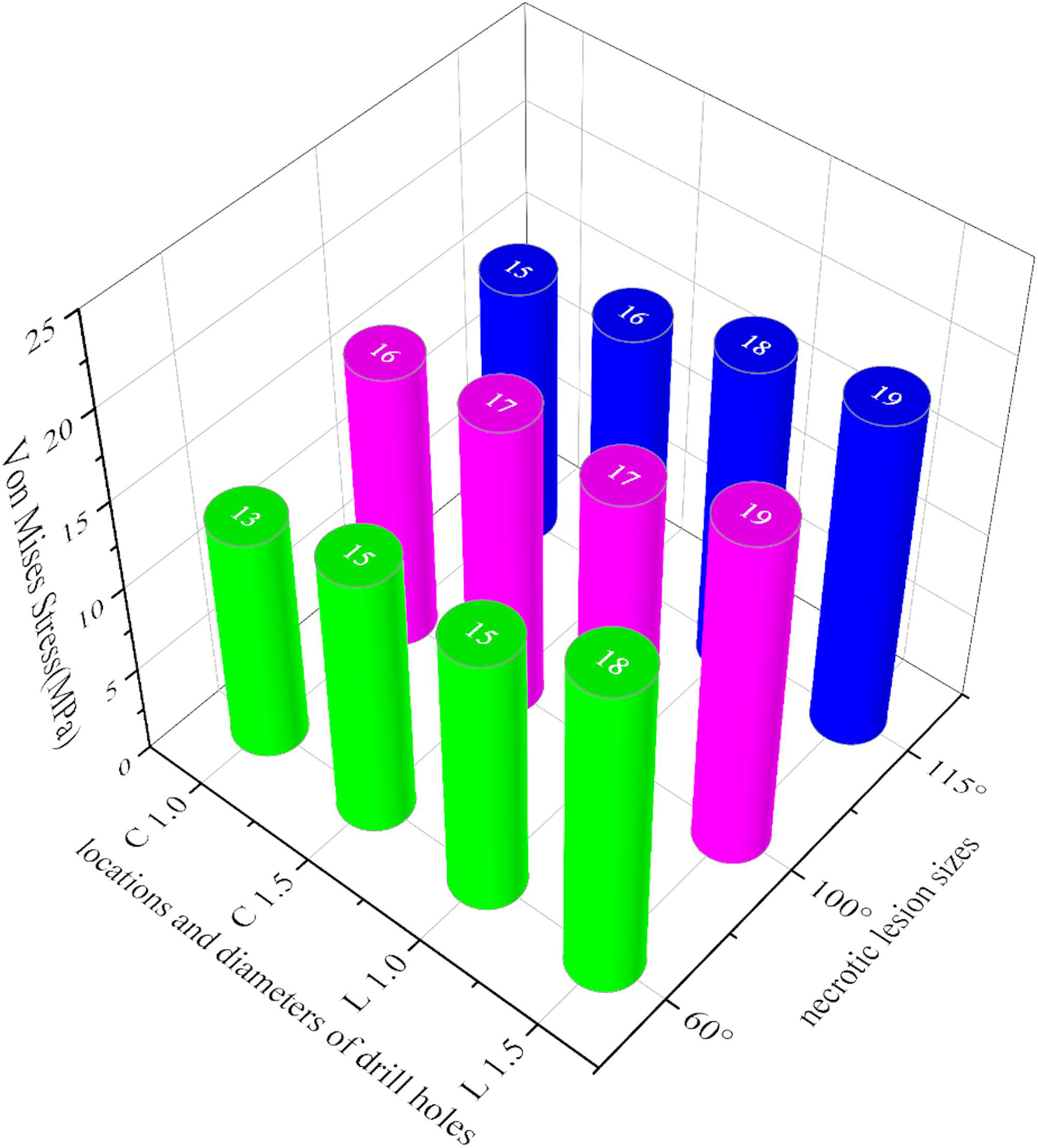
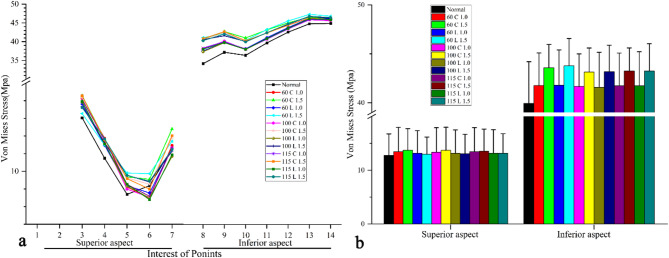
Results: The stress of the superior and inferior edges of femoral neck, entrance, and bone flap increased as drilling diameter increased. The maximum Von Mises stress of proximal femur does not exceed its yield strength with diameter of 1.0 cm, except for diameter of 1.5 cm. The stress of entrance area and bone flap cortex at point L were higher than those at point C with same diameter. Moreover, the stress of femoral neck and entrance area decreased as the range of lesions increased, except for bone flap cortex. Furthermore, the maximum Von Mises stress of proximal femur did not exceed its yield strength with patients standing on one or both feet and walking process (4BW) with drilling diameter of 1.0 cm at points C or L after surgery, except for diameter of 1.5 cm. Meanwhile, the angles reaching to the coronal plane and transverse plane of weight-bearing area through point L with diameter of 1.0 cm were smaller than those through point C.
Conclusions: The optimal parameters of LBT can be selected with a diameter of 1.0 cm at point L. Patients can load partial weight to stimulate the healing of the necrotic area after surgery, but avoid beyond middle foot weight during walking.
Keywords: Finite element analysis; Hip preserving; Lightbulb technique; Optimal parameters; Osteonecrosis of femoral head.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study conforms to the provisions of the Declaration of Helsinki and has been reviewed and approved by the Institutional Review Board of the Affiliated Hospital of Guizhou Medical University (Approval No.2023 − 772). Informed consent was obtained from the participant included in the study. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



Similar articles
-
Biomechanical research of medial femoral circumflex vascularized bone-grafting in the treatment of early-to-mid osteonecrosis of the femoral head: a finite element analysis.J Orthop Surg Res. 2022 Oct 4;17(1):441. doi: 10.1186/s13018-022-03335-7. J Orthop Surg Res. 2022. PMID: 36195938 Free PMC article.
-
Biomechanical analysis of the drilling parameters for early osteonecrosis of the femoral head.Comput Methods Programs Biomed. 2022 Jun;219:106737. doi: 10.1016/j.cmpb.2022.106737. Epub 2022 Mar 8. Comput Methods Programs Biomed. 2022. PMID: 35325669
-
[Finite element analysis for predicting osteonecrosis of the femoral head collapse based on the preserved angles].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023 Nov 15;37(11):1394-1402. doi: 10.7507/1002-1892.202308072. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023. PMID: 37987051 Free PMC article. Chinese.
-
CT Hounsfield units in assessing bone and soft tissue quality in the proximal femur: A systematic review focusing on osteonecrosis and total hip arthroplasty.PLoS One. 2025 Mar 26;20(3):e0319907. doi: 10.1371/journal.pone.0319907. eCollection 2025. PLoS One. 2025. PMID: 40138288 Free PMC article.
-
Femoral osteotomies for the treatment of avascular necrosis of the femoral head.Oper Orthop Traumatol. 2020 Apr;32(2):116-126. doi: 10.1007/s00064-019-00642-x. Epub 2019 Nov 29. Oper Orthop Traumatol. 2020. PMID: 31784775 Review. English.
References
-
- Sato R, Ando W, Fukushima W, Sakai T, Hamada H, Takao M, et al. Epidemiological study of osteonecrosis of the femoral head using the National registry of designated intractable diseases in Japan. Mod Rheumatol. 2022;32(4):808–14. - PubMed
-
- Lamb JN, Holton C, O’Connor P, Giannoudis PV. Avascular necrosis of the hip. BMJ. 2019;365:12178. - PubMed
-
- Chughtai M, Piuzzi NS, Khlopas A, Jones LC, Goodman SB, Mont MA. An evidence-based guide to the treatment of osteonecrosis of the femoral head. Bone Joint J. 2017;99–B(10):1267–79. - PubMed
-
- Erivan R, Riouach H, Villatte G, Pereira B, Descamps S, Boisgard S. Hip preserving surgery for avascular hip necrosis: does terminating exposure to known risk factors improve survival? Phys Sportsmed. 2020;48(3):335–41. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
