

Prognostic value of baseline glucose levels for mortality in patients with cardiogenic shock: a systematic review and meta-analysis
- PMID: 40420156
- PMCID: PMC12105281
- DOI: 10.1186/s13019-025-03483-x
Prognostic value of baseline glucose levels for mortality in patients with cardiogenic shock: a systematic review and meta-analysis
Abstract
Background: Baseline glucose levels have been implicated in the prognosis of critically ill patients. However, the prognostic value of glucose in patients with cardiogenic shock (CS) has not been systematically evaluated. The current study aimed to provide evidence that baseline glucose levels can predict mortality in patients with CS.
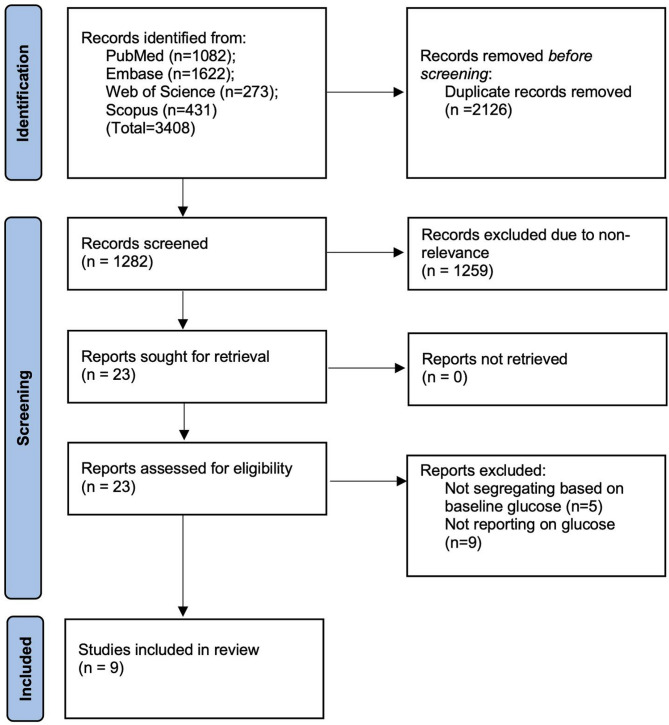
Methods: PubMed, Scopus, Embase and Web of Science were searched from inception to July 31, 2024 for studies assessing mortality after CS based on different baseline glucose levels. Hyperglycemia was defined as a glucose level > 7.8-8 mmol/l. Data were synthesized using "Review Manager" (RevMan; version 5.3; The Cochrane Collaboration).
Results: A total of nine studies were included. Meta-analysis showed that patients with CS who had baseline glucose levels > 7.8-8 mmol/l had a significantly greater risk of early mortality as compared to those with glucose levels < 7.8-8 mmol/l [risk ratio (RR), 1.48; 95% confidence interval (CI), 1.24-1.77; I-squared (I2) = 65%]. Similarly, patients with CS who had baseline glucose levels > 10-11 mmol/l (RR, 1.98; 95% CI, 1.35-2.90; I2 = 82%) and 11.5-12mmol/l (RR, 1.43; 95% CI, 1.19-1.72; I2 = 74%) had significantly greater risk of early mortality as compared to those with lower levels. Severe hyperglycemia (> 16 mmol/l) was also associated with an increased risk of mortality compared with normoglycemia (RR, 1.84; 95% CI, 1.36-2.48; I2 = 78%).
Conclusion: In the present meta-analysis, the elevated risk of mortality was persistent with different glucose cut-offs, suggesting that glucose levels at admission can be useful for risk assessment in patients with CS. Further studies considering diabetes status and other important confounding factors are needed to obtain more evidence.
Keywords: Cardiogenic shock; Diabetes; Glucose; Hyperglycemia; Mortality.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Patient consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures





Similar articles
-
The association of admission blood glucose level with the clinical picture and prognosis in cardiogenic shock - Results from the CardShock Study.Int J Cardiol. 2017 Jan 1;226:48-52. doi: 10.1016/j.ijcard.2016.10.033. Epub 2016 Oct 17. Int J Cardiol. 2017. PMID: 27788389 Clinical Trial.
-
Prognostic impact of baseline glucose levels in acute myocardial infarction complicated by cardiogenic shock—a substudy of the IABP-SHOCK II-trial [corrected].Clin Res Cardiol. 2018 Jun;107(6):517-523. doi: 10.1007/s00392-018-1213-7. Epub 2018 Feb 8. Clin Res Cardiol. 2018. PMID: 29423774 Clinical Trial.
-
Stress hyperglycemia is associated with poor prognosis in critically ill patients with cardiogenic shock.Front Endocrinol (Lausanne). 2024 Sep 5;15:1446714. doi: 10.3389/fendo.2024.1446714. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39301321 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Development of type 2 diabetes mellitus in people with intermediate hyperglycaemia.Cochrane Database Syst Rev. 2018 Oct 29;10(10):CD012661. doi: 10.1002/14651858.CD012661.pub2. Cochrane Database Syst Rev. 2018. PMID: 30371961 Free PMC article.
References
-
- van Diepen S, Katz JN, Albert NM, et al. Contemporary management of cardiogenic shock: A scientific statement from the American heart association. Circulation. 2017;136:e232–68. - PubMed
-
- Berg DD, Bohula EA, Morrow DA. Epidemiology and causes of cardiogenic shock. Curr Opin Crit Care. 2021;27:401–8. - PubMed
-
- Kolte D, Khera S, Dabhadkar KC, et al. Trends in coronary angiography, revascularization, and outcomes of cardiogenic shock complicating Non-ST-Elevation myocardial infarction. Am J Cardiol. 2016;117:1–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
