

Fentanyl or esketamine for traumatic pain (FORE-PAIN) trial: study protocol for a double-blind multi-arm randomized non-inferiority trial
- PMID: 40420189
- PMCID: PMC12105219
- DOI: 10.1186/s13063-025-08869-9
Fentanyl or esketamine for traumatic pain (FORE-PAIN) trial: study protocol for a double-blind multi-arm randomized non-inferiority trial
Abstract
Background: Although fentanyl and esketamine, administered intravenously (IV) or intranasally (IN), are standard of care for treatment of acute traumatic pain in the prehospital setting in the Netherlands, comparative evidence regarding their efficacy and safety is lacking. Therefore, this study aims to assess the efficacy and safety of fentanyl IN, esketamine IV and esketamine IN as compared to fentanyl IV for management of acute traumatic pain in the prehospital setting.
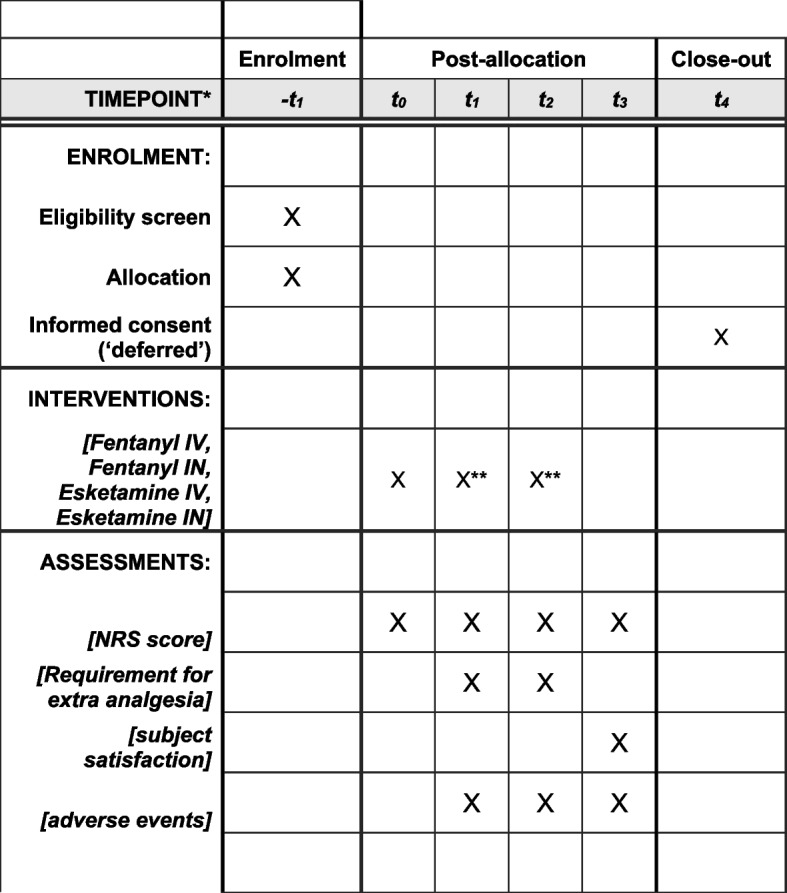
Methods: This is a double-blind, monocenter, multi-arm, randomized non-inferiority trial in the prehospital setting in the Netherlands. Adult subjects receiving emergency care from Emergency Medical Services Ambulance Amsterdam and suffering from acute severe traumatic pain are randomized in an 1:1:1:1 ratio to receive fentanyl IV (1.0 µg/kg), fentanyl IN (1.25 µg/kg), esketamine IV (0.2 mg/kg), or esketamine IN (0.625 mg/kg). The primary endpoint is the reduction in Numeric Rating Scale (NRS, 0-10) score at 10 min after first administration of study medication. The prespecified non-inferiority margin is 1.0 for the between-group absolute difference in primary outcome. The primary endpoint is analyzed according to the intention-to-treat and per-protocol principles conforming to recommendations for non-inferiority analysis. Other endpoints include reduction in NRS score at other timepoints, need for additional analgesia, patient satisfaction, and adverse events.
Discussion: This trial is one of few double-blind randomized controlled trials in the prehospital setting and aims to answer questions that have relevance to prehospital practice. Research in a prehospital emergency setting also comes with challenges, including concerns about prehospital data quality, limited research experience among personnel and a limited timeframe for data collection and follow-up. Also, informed consent needs to be deferred.
Trial registration: ClinicalTrials.gov NCT06051227. Registered on 9 September 2023.
Keywords: Acute pain; Administration; Analgesia; Emergency medical services; Esketamine; Fentanyl; Intranasal; Intravenous; Wounds and injuries.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate {24}: The Institutional Review Board of the Amsterdam UMC has approved this trial. Informed consent is deferred until after arrival at the hospital, after which all subjects will be approached to provide informed consent, either electronically or written. Consent for publication {32}: Not applicable. Competing interests {28}: The authors declare that they have no competing interests.
Figures
References
-
- Dhir S, v Sondekoppam R, Ganapathy S. Pharmacologic management of acute pain in trauma. In: Smith CE, editor. Trauma anesthesia (2nd ed): Cambridge University Press; 2015. p. 244-66.
-
- Berben SA, Meijs TH, van Dongen RT, van Vugt AB, Vloet LC, Mintjes-de Groot JJ, et al. Pain prevalence and pain relief in trauma patients in the Accident & Emergency department. Injury. 2008;39(5):578–85. - PubMed
-
- Berben SA, Schoonhoven L, Meijs TH, van Vugt AB, van Grunsven PM. Prevalence and relief of pain in trauma patients in emergency medical services. Clin J Pain. 2011;27(7):587–92. - PubMed
-
- Savoia G, Coluzzi F, Di Maria C, Ambrosio F, Della Corte F, Oggioni R, et al. Italian Intersociety Recommendations on pain management in the emergency setting (SIAARTI, SIMEU, SIS 118, AISD, SIARED, SICUT, IRC). Minerva Anestesiol. 2015;81(2):205–25. - PubMed
-
- Pre-hospital Emergency Care Council (PHECC). Clinical Practice Guidelines: Advanced Paramedic (7th ed) [Online]. Naas, Ireland: PHECC; 2021 [updated June 2023; cited 2024 16 January]. Available from: https://www.phecit.ie/PHECC/Clinical_Resources/Clinical_Practice_Guideli....
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
