

Effects of external fixator-assisted acute angulation on arterial diameter: a cadaveric model
- PMID: 40420237
- PMCID: PMC12107902
- DOI: 10.1186/s13018-025-05948-0
Effects of external fixator-assisted acute angulation on arterial diameter: a cadaveric model
Abstract
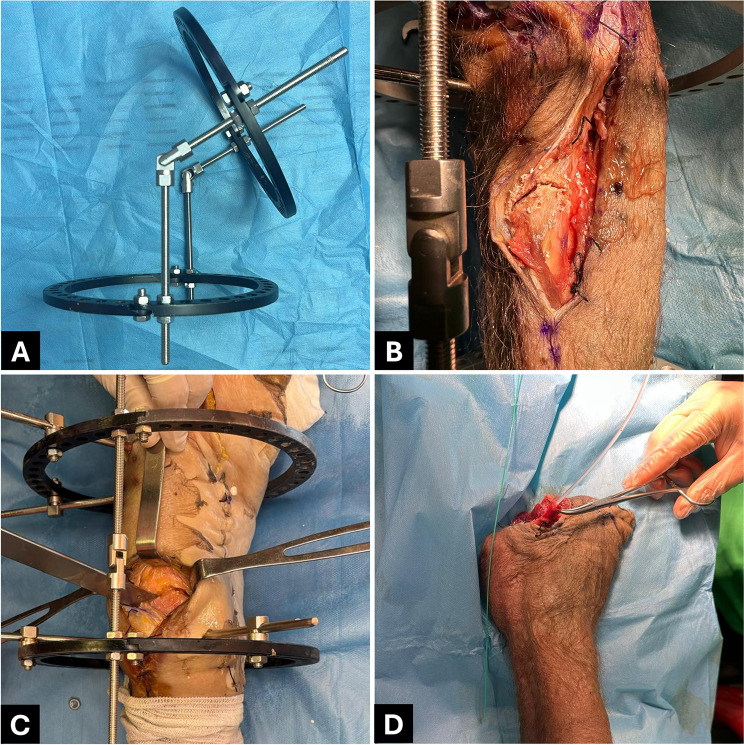
Background: Open fractures with bone and soft tissue loss pose significant challenges in orthopedic surgery. External fixator-assisted techniques, such as acute angulation and shortening, have been proposed to facilitate wound closure. However, the vascular implications of these techniques remain unclear. This cadaveric study aimed to evaluate the effect of acute angulation on arterial narrowing at the proximal tibia and distal femur, identifying angulation thresholds and comparing the vascular tolerance between these anatomical sites.
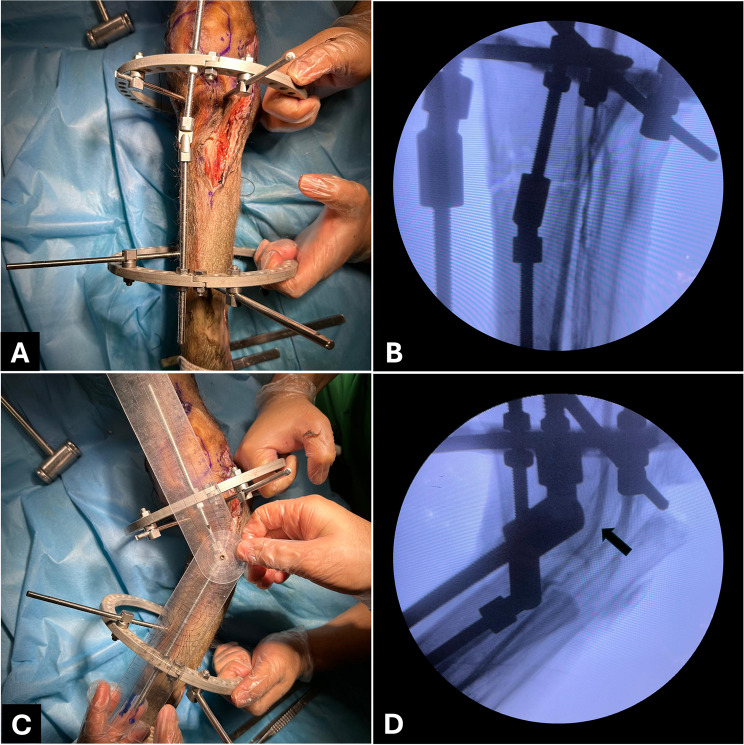
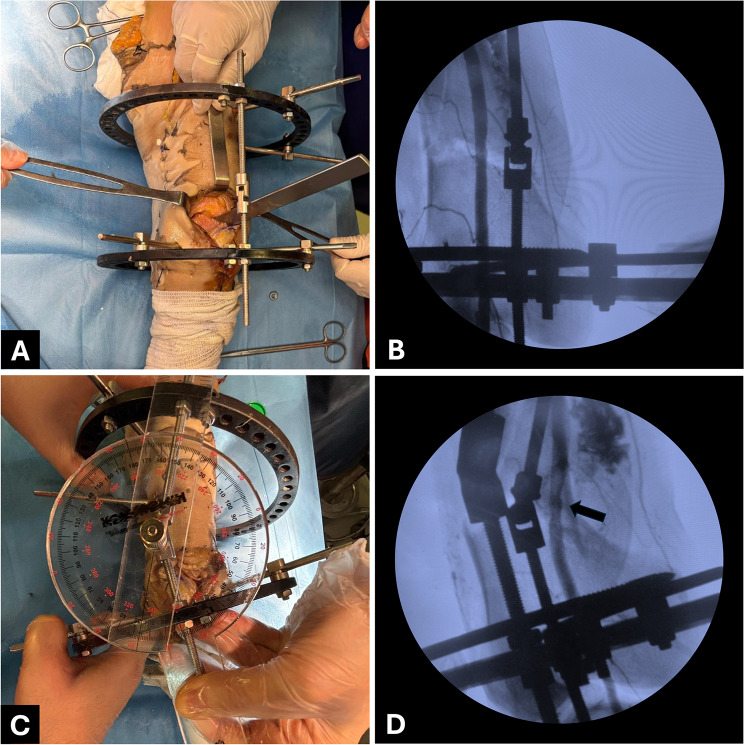
Methods: Eight lower extremities from four fresh-frozen cadavers were used. Osteotomies were performed at the distal femoral and proximal tibial metaphyses. An Ilizarov circular external fixator provided controlled angulation in varus, valgus, procurvatum, and recurvatum directions. A contrast agent was used for vascular visualization under fluoroscopy. Angulation was gradually increased until arterial narrowing was observed, and the critical angles were recorded.
Results: In the proximal tibia, the mean angulation thresholds for arterial narrowing were 45.5° in varus, 26.5° in valgus, 33.8° in procurvatum, and 13.5° in recurvatum. In the distal femur, arterial narrowing occurred at 27° in varus, 32.3° in valgus, 52° in procurvatum, and 22° in recurvatum. Varus angulation was significantly better tolerated at the tibia (p = 0.0286), while procurvatum (p = 0.0294) and recurvatum (p = 0.0286) were better tolerated at the femur. No significant difference was found in valgus angulation (p = 0.559).
Conclusions: The tibia demonstrated higher tolerance for varus angulation, while the femur allowed greater procurvatum and recurvatum before vascular compromise. Recurvatum deformities in the tibia resulted in the earliest arterial narrowing, suggesting a higher risk of vascular complications. These findings provide critical insight for surgeons performing external fixator-assisted soft tissue coverage, helping optimize angulation strategies to prevent vascular complications.
Keywords: External fixators; Fractures; Ilizarov technique; Open; Soft tissue injuries; Thrombosis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for the study was obtained from the Ethics Committee of Çukurova University Faculty of Medicine with decision number 39, taken at meeting number 151 on January 3, 2025. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Molding Spica Casts to Maintain Alignment of Femur Fractures.J Pediatr Orthop. 2018 May/Jun;38(5):e267-e270. doi: 10.1097/BPO.0000000000001165. J Pediatr Orthop. 2018. PMID: 29521935
-
Comprehensive treatment of late-onset tibia vara.J Bone Joint Surg Am. 2005 Jul;87(7):1561-70. doi: 10.2106/JBJS.02276. J Bone Joint Surg Am. 2005. PMID: 15995124
-
Cementless, Cruciate-Retaining Primary Total Knee Arthroplasty Using Conventional Instrumentation: Technical Pearls and Intraoperative Considerations.JBJS Essent Surg Tech. 2024 Sep 13;14(3):e23.00036. doi: 10.2106/JBJS.ST.23.00036. eCollection 2024 Jul-Sep. JBJS Essent Surg Tech. 2024. PMID: 39280965 Free PMC article.
-
Acute Correction of Multiplanar Proximal Tibial Deformity Utilizing Fixator-Assisted Intramedullary Nailing.JBJS Essent Surg Tech. 2022 Aug 31;12(3):e21.00045. doi: 10.2106/JBJS.ST.21.00045. eCollection 2022 Jul-Sep. JBJS Essent Surg Tech. 2022. PMID: 36816522 Free PMC article.
-
[Corrective osteotomies around the knee joint using hexapods].Oper Orthop Traumatol. 2024 Apr;36(2):83-95. doi: 10.1007/s00064-023-00836-4. Epub 2023 Nov 10. Oper Orthop Traumatol. 2024. PMID: 37947855 Review. German.
References
-
- Jones CM, Roberts JM, Sirlin EA, Cavanaugh GA, Anagnostakos JP, Hauck RM et al. Acute limb shortening or creation of an intentional deformity to aid in soft tissue closure for IIIB/IIIC open tibia fractures. Journal of Plastic, Reconstructive and Aesthetic Surgery [Internet]. 2021;74:2933–40. Available from: 10.1016/j.bjps.2021.03.105 - PubMed
-
- Sen C, Kocaoglu M, Eralp L, Gulsen M, Cinar M. Bifocal compression-distraction in the acute treatment of grade III open tibia fractures with bone and soft-tissue loss: A report of 24 cases. J Orthop Trauma. 2004;18:150–7. - PubMed
-
- Lahoti O, Findlay I, Shetty S, Abhishetty N. Intentional deformation and closure of soft tissue defect in open tibial fractures with a Taylor Spatial frame-a simple technique. J Orthop Trauma. 2013;27:451–6. - PubMed
-
- Gulsen M, özkan C. Angular shortening and delayed gradual distraction for the treatment of asymmetrical bone and soft tissue defects of Tibia: A case series. J Trauma. 2009;66:E61–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
