

Screening for atrial fibrillation with or without general practice involvement: a controlled study
- PMID: 40420263
- PMCID: PMC12105410
- DOI: 10.1186/s12875-025-02878-y
Screening for atrial fibrillation with or without general practice involvement: a controlled study
Abstract
Background: There has been a drive to increase atrial fibrillation (AF) detection in general practice. However, one-off, opportunistic testing can miss paroxysmal AF and requires significant resource. Paroxysmal AF can be detected through screening that involves repeated ECGs over a period of time, although it is unclear whether screening would need to be led by general practice, and how much support participants require. We aimed to investigate whether AF screening can be delivered remotely by a centralised administration instead of general practice, and to determine the level of support required.
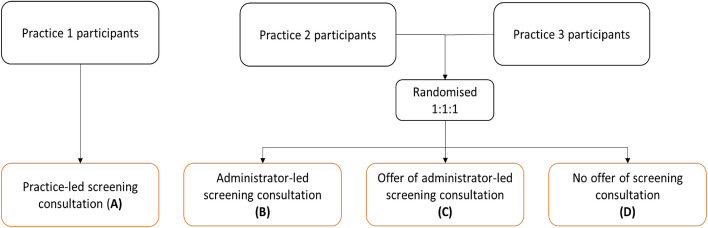
Methods: We undertook a controlled comparator study with secondary randomisation in three English general practices. We invited people aged ≥ 70 years to use a hand-held ECG device four times daily for three weeks. Participants were allocated to practice-led or administrator-led screening, with administrator-led support randomised to three different levels. We compared quantity and quality of ECGs obtained in each arm. The primary outcome was proportion of screened participants who recorded ≥ 56 adequate-quality ECGs (2/3 of possible ECGs).
Results: Of 288 screened participants, 59 participants received practice-led screening with a telephone consultation to explain the device. The remainder received administrator-led screening: 81 were automatically given a consultation; 74 were offered a consultation, and 74 were not offered a consultation. Most screened participants (280/288, 97.2%) recorded ≥ 56 adequate-quality ECGs. This proportion did not vary significantly between practice-led and administrator-led screening (100.0% vs. 98.8%), or between support levels (94.6% to 98.8%). Practice-led screening led to slightly more adequate-quality ECGs (mean: 83.9 vs 78.3, p < 0.001).
Conclusions: AF screening can be successfully delivered remotely, outside general practice, with minimal support.
Keywords: Atrial fibrillation; Feasibility study; Primary care; Remote deliver; Screening.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This feasibility study received ethical approval from the London – Central NHS Research Ethics Committee (19/LO/1597). Written informed consent to participate was obtained from all participants in the study. The research was conducted in accordance with the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: All authors are undertaking the SAFER study named in the paper. JM has performed consultancy work for BMS/Pfizer and Omron. FDRH reports occasional consultancy for BMS/Pfizer, Bayer and BI over the last five years. GYHL: Consultant and speaker for BMS/Pfizer, Boehringer Ingelheim, Daiichi-Sankyo, Anthos. No fees are received personally. SJG has received honoraria from Astra Zeneca for lecturer at postgraduate educational meetings for primary care teams about type 2 diabetes. BF has received speaker fees, honoraria, and non-financial support from the BMS and Pfizer Alliance; and loan devices for investigator initiated studies from Alivecor: all were unrelated to the present study, but related to screening for AF. PHC has performed consultancy work for Cambridge University Technical Services and has received honoraria from IOP Publishing and Emory University (the latter not received personally).
Figures


References
-
- NHS England and NHS Improvement. The NHS Long Term Plan. NHS; 2019. Available from: https://www.longtermplan.nhs.uk/online-version/chapter-2-more-nhs-action....
-
- King S, Fitzgerald A, Bartlett C, Mahon J, Arber M, Carr E, et al. Evidence Summary for Screening for Atrial Fibrillation in Adults: External review against programme appraisal criteria for the UK National Screening Committee. UK National Screening Committee; 2019. Available from: https://legacyscreening.phe.org.uk/policydb_download.php?doc=968.
-
- Wessex Academic Health Science Network (AHSN). Independent Evaluation of the AHSN Network mobile ECG roll-out programme; 2019. Available from: https://wessexahsn.org.uk/img/insight_reports/Mobile%20ECG%20Evaluation%....
-
- National Institute for Health and Care Excellence. Atrial fibrillation: diagnosis and management (ng196). National Institute of Health and Care Excellence; 2021. Available from: https://www.nice.org.uk/guidance/NG196.
Publication types
MeSH terms
Grants and funding
- RP-PG-0217-20007/National Institute for Health and Care Research
- RP-PG-0217-20007/National Institute for Health and Care Research
- RP-PG-0217-20007/National Institute for Health and Care Research
- RP-PG-0217-20007/National Institute for Health and Care Research
- RP-PG-0217-20007/National Institute for Health and Care Research
LinkOut - more resources
Full Text Sources
Medical