

Validity and Responsiveness of Balance Measurements Using Posturography in Patients With Immune-Mediated Neuropathies
- PMID: 40420525
- PMCID: PMC12107020
- DOI: 10.1111/jns.70031
Validity and Responsiveness of Balance Measurements Using Posturography in Patients With Immune-Mediated Neuropathies
Abstract
Background and aims: Validated objective measures for balance in immune mediated neuropathies are lacking. In this study, we investigated the clinimetric properties of posturography using a force platform, a quantitative assessment of postural control.
Methods: We assessed patients with chronic inflammatory demyelinating polyneuropathy (CIDP) and IgM-related polyneuropathy (IgM-PNP) using sway parameters (path, area and amplitude) measured at multiple time points. Validity was investigated by assessing differences in sway path between patients with and without reported balance symptoms and by assessing correlations of sway path with (established) impairment measures related to balance, disability and quality of life (QoL). Responsiveness was assessed by means of an anchor-based approach, using a patient anchor and two disability scales.
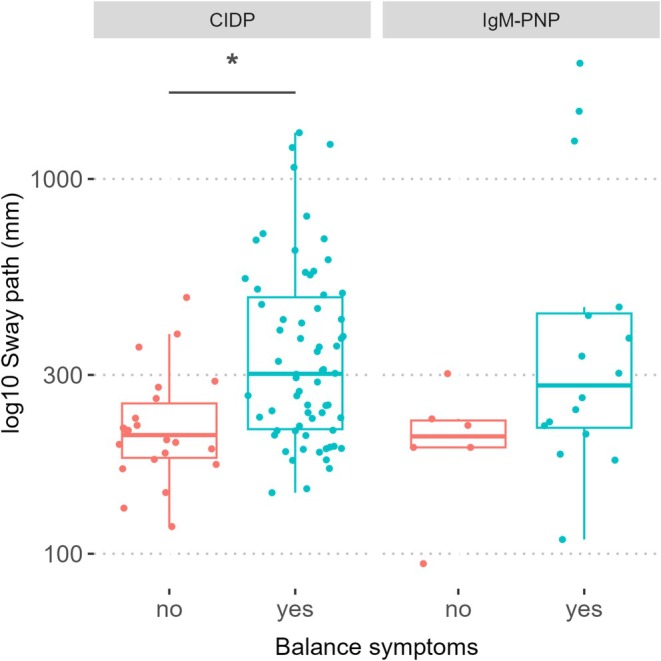
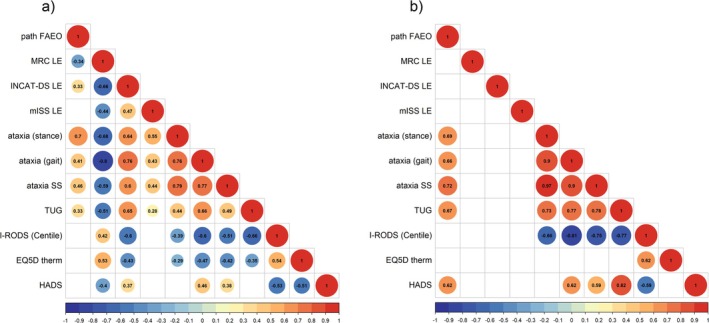
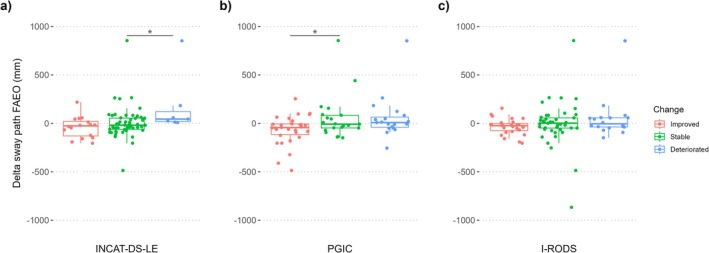
Results: We included 52 CIDP and 13 IgM-PNP patients. In CIDP, sway path was 25% longer in patients reporting balance symptoms relative to patients without balance symptoms (p = 0.03). There was excellent reliability between consecutive measurements in both CIDP and IgM-PNP. Moderate to good correlations were observed between sway path and an ataxia scale (CIDP: Spearman's ρ = 0.46, 95% CI: 0.2-0.69; IgM-PNP: Spearman's ρ = 0.72, 95% CI: 0.28-0.96) while correlations with related disability measures and QoL were poor. Changes in sway parameters over time were not consistently associated with changes in other outcome measures.
Interpretation: Posturography measurements showed poor validity and responsiveness. Therefore, despite excellent reliability, using a force platform in clinical practice or trials for immune-mediated neuropathies cannot be recommended.
Keywords: CIDP; IgM‐related polyneuropathy; balance; posturography; responsiveness; validity.
© 2025 The Author(s). Journal of the Peripheral Nervous System published by Wiley Periodicals LLC on behalf of Peripheral Nerve Society.
Figures
Similar articles
-
Quality of life in inflammatory neuropathies: the IN-QoL.J Neurol Neurosurg Psychiatry. 2018 Mar;89(3):256-262. doi: 10.1136/jnnp-2017-316634. Epub 2017 Oct 6. J Neurol Neurosurg Psychiatry. 2018. PMID: 28986470
-
Changing outcome in inflammatory neuropathies: Rasch-comparative responsiveness.Neurology. 2014 Dec 2;83(23):2124-32. doi: 10.1212/WNL.0000000000001044. Epub 2014 Nov 5. Neurology. 2014. PMID: 25378677
-
Postural balance and visual dependence in patients with demyelinating neuropathies differ between acquired and hereditary etiologies.Rev Neurol (Paris). 2025 Jan-Feb;181(1-2):98-105. doi: 10.1016/j.neurol.2024.10.002. Epub 2024 Oct 28. Rev Neurol (Paris). 2025. PMID: 39462724
-
Patient-Reported Outcome Measures for Assessing Health-Related Quality of Life in Patients With Polyneuropathies, Focusing on Guillain-Barré Syndrome and Chronic Inflammatory Demyelinating Polyneuropathy: A Systematic Review of Measurement Properties.J Peripher Nerv Syst. 2025 Jun;30(2):e70022. doi: 10.1111/jns.70022. J Peripher Nerv Syst. 2025. PMID: 40366569 Free PMC article. Review.
-
Chronic Inflammatory Demyelinating Polyradiculoneuropathy and Its Variants.Continuum (Minneap Minn). 2020 Oct;26(5):1205-1223. doi: 10.1212/CON.0000000000000907. Continuum (Minneap Minn). 2020. PMID: 33002999 Review.
References
-
- Westblad M. E., Forsberg A., and Press R., “Disability and Health Status in Patients With Chronic Inflammatory Demyelinating Polyneuropathy,” Disability and Rehabilitation 31, no. 9 (2009): 720–725. - PubMed
-
- Ryltoft A. K., Al‐Zuhairy A., Sindrup S. H., Andersen H., and Markvardsen L. K., “Quality of Life in Chronic Inflammatory Demyelinating Polyneuropathy Patients Treated With Subcutaneous Immunoglobulin,” Acta Neurologica Scandinavica 142, no. 6 (2020): 637–640. - PubMed
-
- Inglis J. T., Horak F. B., Shupert C. L., and Jones‐Rycewicz C., “The Importance of Somatosensory Information in Triggering and Scaling Automatic Postural Responses in Humans,” Experimental Brain Research 101, no. 1 (1994): 159–164. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
