

Distinct immunity dynamics of natural killer cells in mild and moderate COVID-19 cases during the Omicron variant phase
- PMID: 40421029
- PMCID: PMC12104262
- DOI: 10.3389/fimmu.2025.1594296
Distinct immunity dynamics of natural killer cells in mild and moderate COVID-19 cases during the Omicron variant phase
Abstract
Background: The SARS-CoV-2 Omicron variant is associated with milder COVID-19 symptoms than previous strains. This study analyzed alterations in natural killer (NK) cell-associated immunity dynamics in mild and moderate COVID-19 cases during the Omicron phase of the COVID-19 pandemic.
Methods: We conducted a retrospective observational cohort study of patients aged ≥16 with confirmed SARS-CoV-2 infection who were hospitalized at Tottori University Hospital between January 2022 and May 2022. A total of 27 patients were included in the analysis. Of these, 11 and 16 were diagnosed with mild and moderate COVID-19, respectively, based on the Japanese COVID-19 clinical practice guideline. Peripheral blood NK cell subsets and surface markers, including the activating receptor NKG2D and the inhibitory receptor TIGIT, as well as serum levels of 24 immunoregulatory markers, such as cytokines and cytotoxic mediators, were measured at admission and recovery. In addition, to explore immune patterns associated with disease severity, differences in 24 serum markers and soluble UL16-binding protein 2 (sULBP2) at the clinically most symptomatic time point during hospitalization were visualized using a volcano plot and analyzed with Spearman's rank correlation analysis and principal component analysis (PCA).
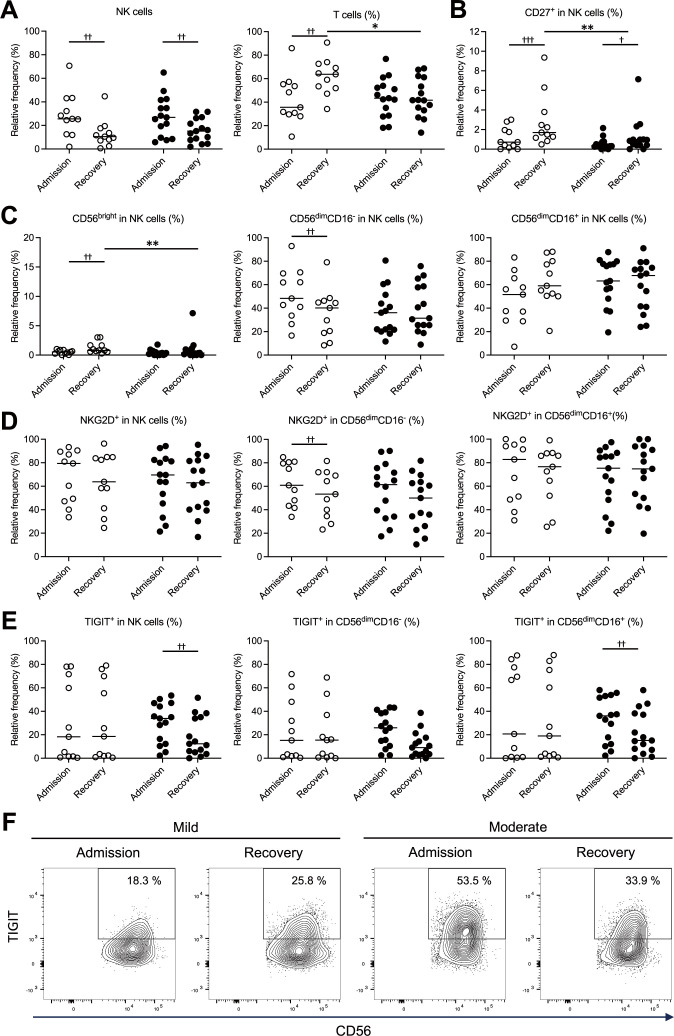
Results: Patients with mild COVID-19 exhibited expanded subsets of unconventional CD56dimCD16- NK cells with elevated NKG2D expression and lower levels of cytotoxic mediators (granzyme A, granzyme B, and granulysin). In contrast, patients with moderate disease exhibited NK cell exhaustion, characterized by upregulation of TIGIT, along with increased levels of NK cell-associated cytokines and cytotoxic mediators. The volcano plot identified that the patients with moderate COVID-19 exhibited significantly elevated IL-6 and sULBP2 levels. Spearman's rank correlation analysis revealed that IL-6, IFN-γ, soluble Fas, and CXCL8 were correlated with increased sULBP2. The PCA identified distinct clusters based on disease severity.
Conclusions: The results of study highlight the differences in NK cell-associated immune alterations between mild and moderate COVID-19 cases. Elevated IL-6 and sULBP2 levels, along with their correlations with inflammatory mediators, reflects differences in immune response based on disease severity. These findings provide insight into the immune response to infection caused by the Omicron variant of SARS-CoV-2 and improve our understanding of its immunological features.
Keywords: COVID-19; NKG2D; Omicron variant; TIGIT; ULBP2; cytokines; disease severity; natural killer cells.
Copyright © 2025 Nishikawa, Yamaguchi, Shofiudin, Mimura, Takata, Mihara, Kawakami, Doi, Matsuda, Kato, Okamoto, Mukuda, Kinoshita, Okada, Kitaura, Nakamoto, Noma, Endo, Yamasaki and Chikumi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






Similar articles
-
Integrated analysis of circulating immune cellular and soluble mediators reveals specific COVID19 signatures at hospital admission with utility for prediction of clinical outcomes.Theranostics. 2022 Jan 1;12(1):290-306. doi: 10.7150/thno.63463. eCollection 2022. Theranostics. 2022. PMID: 34987646 Free PMC article.
-
Elevated Exhaustion Levels of NK and CD8+ T Cells as Indicators for Progression and Prognosis of COVID-19 Disease.Front Immunol. 2020 Oct 14;11:580237. doi: 10.3389/fimmu.2020.580237. eCollection 2020. Front Immunol. 2020. PMID: 33154753 Free PMC article.
-
Elevated levels of cell-free NKG2D-ligands modulate NKG2D surface expression and compromise NK cell function in severe COVID-19 disease.Front Immunol. 2024 Feb 12;15:1273942. doi: 10.3389/fimmu.2024.1273942. eCollection 2024. Front Immunol. 2024. PMID: 38410511 Free PMC article.
-
A systematic meta-analysis of immune signatures in patients with COVID-19.Rev Med Virol. 2021 Jul;31(4):e2195. doi: 10.1002/rmv.2195. Epub 2020 Nov 20. Rev Med Virol. 2021. PMID: 34260780 Free PMC article.
-
Dynamics of Innate Immunity in SARS-CoV-2 Infections: Exploring the Impact of Natural Killer Cells, Inflammatory Responses, Viral Evasion Strategies, and Severity.Cells. 2025 May 22;14(11):763. doi: 10.3390/cells14110763. Cells. 2025. PMID: 40497938 Free PMC article. Review.
Cited by
-
NK Cells: A Powerful Squad Versus SARS-CoV-2.Int J Mol Sci. 2025 Jul 6;26(13):6500. doi: 10.3390/ijms26136500. Int J Mol Sci. 2025. PMID: 40650276 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous