

Analyzing the characteristics of Otitis media with effusion following SARS-CoV-2 infection in China
- PMID: 40421276
- PMCID: PMC12104189
- DOI: 10.3389/fsurg.2025.1515724
Analyzing the characteristics of Otitis media with effusion following SARS-CoV-2 infection in China
Abstract
Objective: This study investigates the characteristics of Otitis Media with Effusion (OME) secondary to the SARS-CoV-2 pandemic, and examines whether SARS-CoV-2 is present in middle ear effusions (MEE).
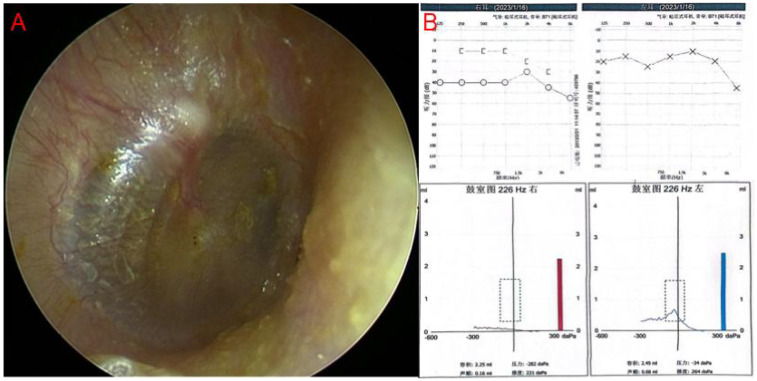
Methods: We analyzed patients diagnosed with SARS-CoV-2 who presented with ear fullness between December 15, 2022, and January 20, 2023. After obtaining a detailed medical history and conducting audiometric assessments, we confirmed OME and performed tympanocentesis to test for SARS-CoV-2 in the MEE following informed consent. Post-procedure, patients received nasal decongestants and oral/nasal corticosteroids. Follow-up consultations, tympanic membrane examinations, and audiometric evaluations were conducted 2-4 weeks later, with a final assessment at three months.
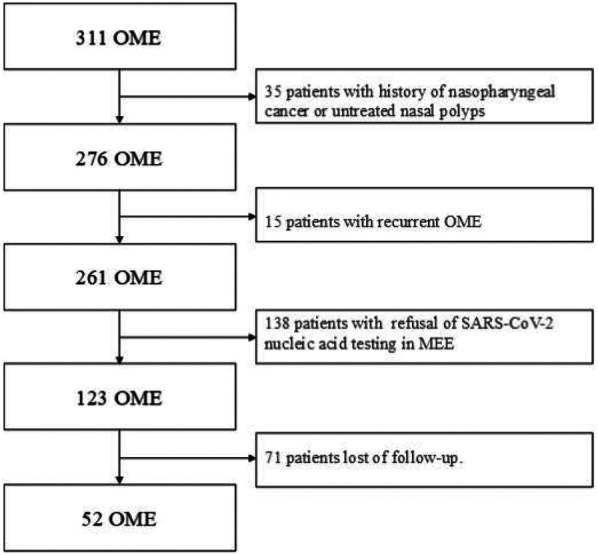
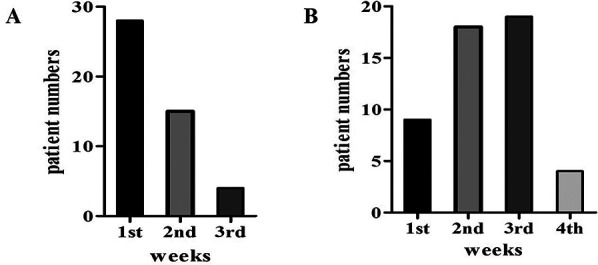
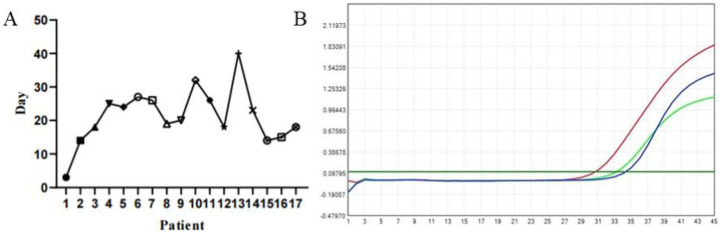
Results: Our clinic recorded 311 OME cases during the study period, accounting for 9.5% of all patients-a significant increase from 2.2% the previous year and 2.5% the following year. The peak incidence occurred one week post-infection. Among the 311 patients, 52 underwent tympanocentesis (33 males, 19 females). 20 patients had bilateral onset, while 32 had unilateral onset. 31 patients were cured after a single tympanocentesis, whereas 21 required two or more procedures. 17 patients tested positive for SARS-CoV-2 in the MEE, but only one simultaneously tested positive in nasal secretions. At the three-month follow-up, 59.6% of patients were cured, 30.8% showed improvement without full recovery, and 9.6% had no improvement. Factors such as poor mastoid pneumatization, nasopharyngeal obstruction, and comorbidities (hypertension, diabetes) affected treatment efficacy. Among the 52 patients, 37 had conductive hearing loss (CHL), and 15 had mixed hearing loss (MHL).
Conclusions: SARS-CoV-2 contributes to OME, primarily affecting one ear. The virus persists longer in MEE than in the upper respiratory tract, suggesting slower viral clearance in the middle ear compared to the nasopharynx. Conductive hearing loss (CHL) is the most common type post-infection, but mixed hearing loss (MHL) can also occur, particularly in older patients, with less favorable outcomes compared to CHL.
Keywords: COVID-19; SARS-CoV-2; conductive hearing loss; middle ear effusion (MEE); mixed hearing loss; otitis media with effusion (OME).
© 2025 Li, Liu, Tan, Zeng, Iqbal and Jiang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous