

Efficacy of acupuncture as adjunctive therapy for patients with acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis
- PMID: 40421292
- PMCID: PMC12104076
- DOI: 10.3389/fmed.2025.1513888
Efficacy of acupuncture as adjunctive therapy for patients with acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is a highly prevalent and potentially fatal respiratory condition. Acute exacerbations can accelerate lung function decline and increase mortality. Acupuncture has been increasingly used as an adjunctive treatment for respiratory diseases, but its effectiveness in acute exacerbations of COPD (AECOPD) remains controversial. Existing evaluations on this topic are limited in scope and depth. This study aimed to provide a more comprehensive review to evaluate the effectiveness of acupuncture as an adjuvant treatment for acute exacerbations of chronic obstructive pulmonary disease.
Study design: Systematic review and meta-analysis of existing randomized controlled trials on acupuncture-assisted treatment of acute exacerbation of chronic obstructive pulmonary disease (AECOPD).
Methods: We included randomized controlled trials (RCTs) comparing acupuncture combined with conventional Western medicine to conventional Western medicine alone in patients with acute exacerbations of COPD (AECOPD). Our literature search covered ten databases, including PubMed and Web of Science ect., up until March 2025. The primary outcome was the effective rate, while secondary outcomes included lung function (FEV1%, FEV1/FVC%, FEV1), arterial blood gas analysis (PaO2, PaCO2, SaO2), the 6-min walk test (6MWT), COPD Assessment Test (CAT), modified Medical Research Council (mMRC) scale, and success rate of weaning. Data were extracted from eligible studies, and statistical analysis was performed using RevMan 5.3 and Stata 16.0. Risk of bias and evidence quality were assessed using Cochrane tools and GRADE methodology.
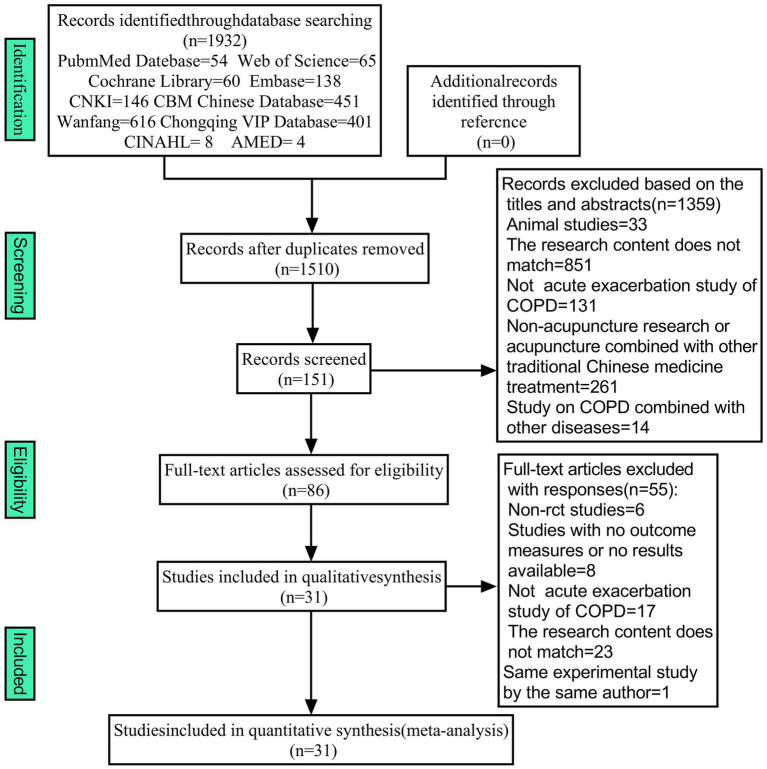
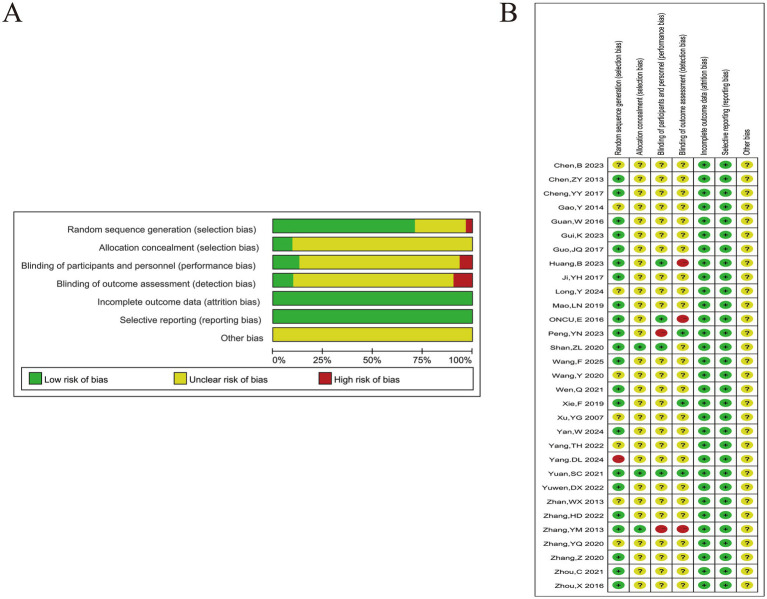
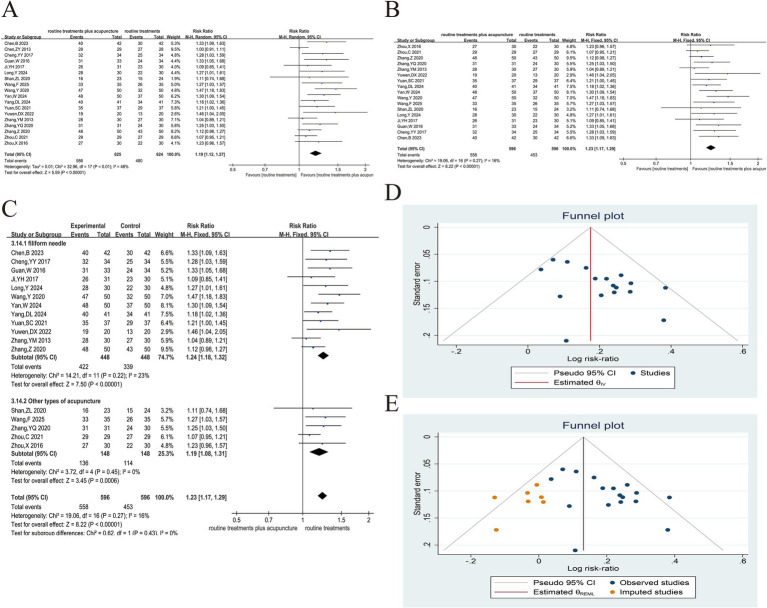
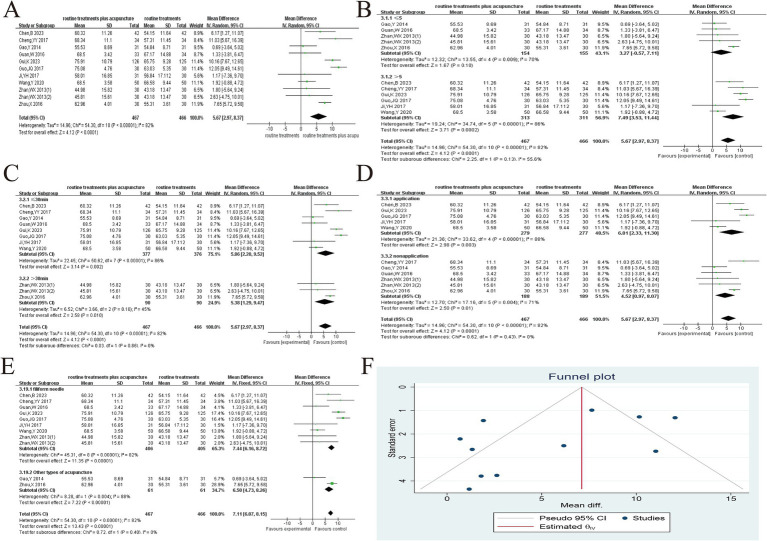
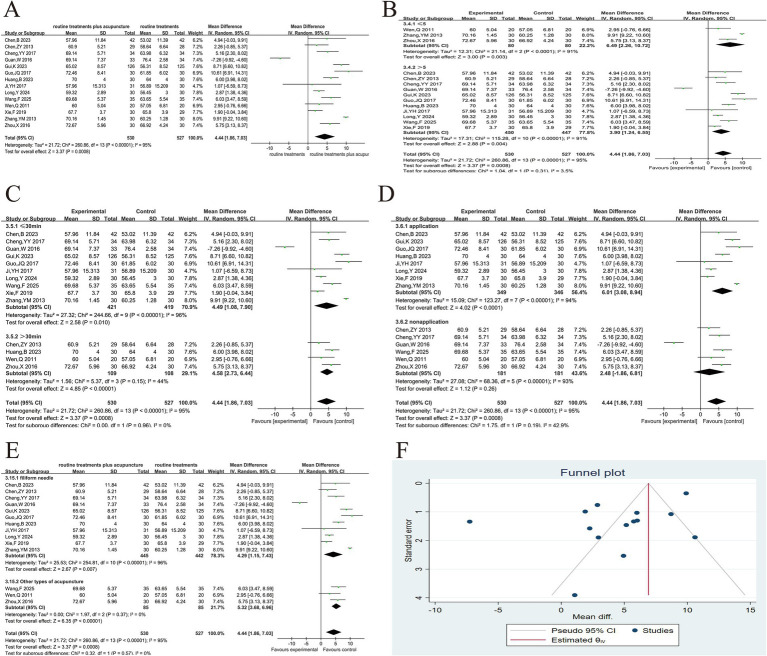
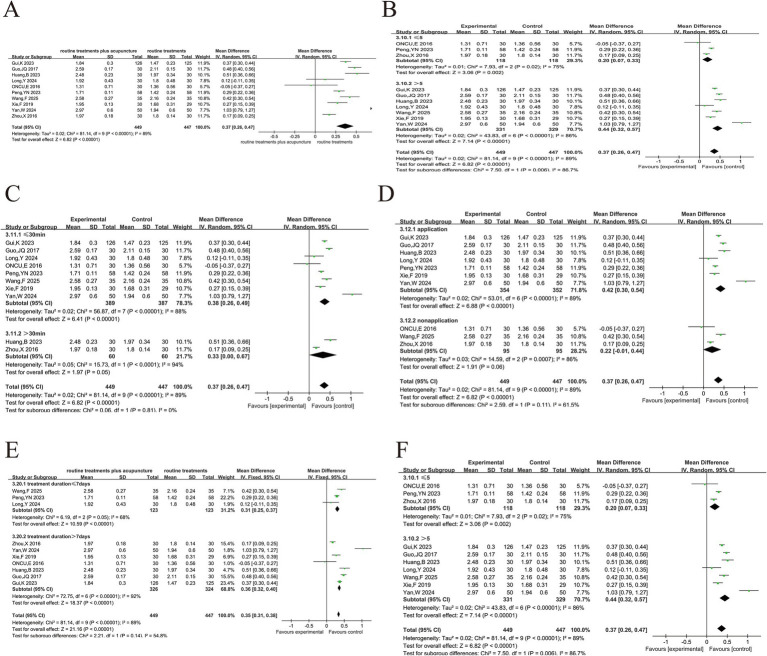
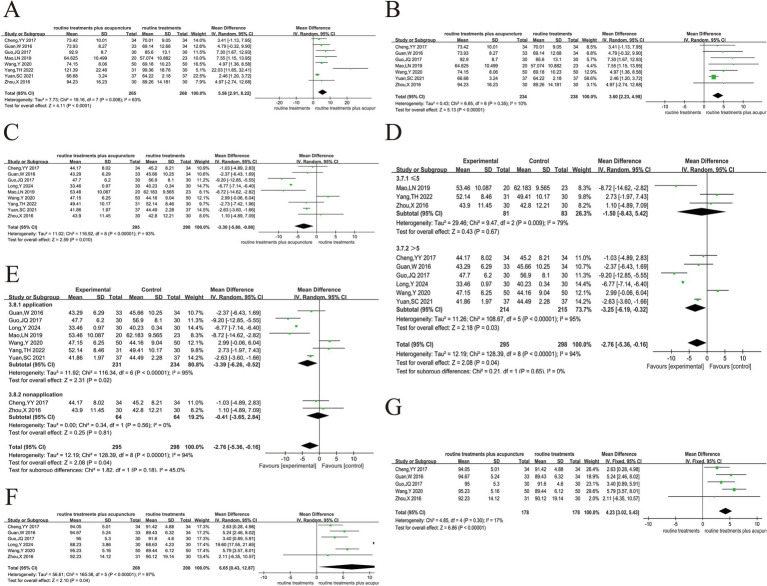
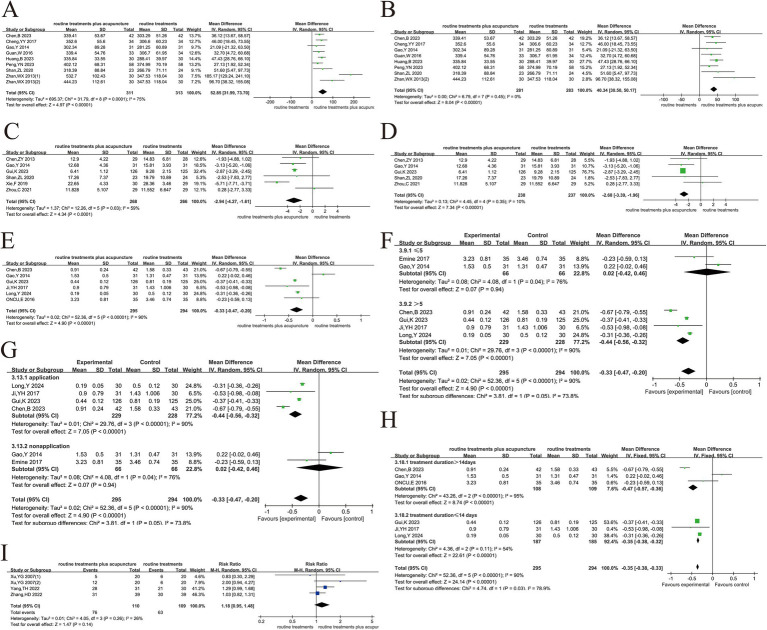
Results: The study included 31 randomized controlled trials (RCTs) with 2,299 participants. The studies were primarily conducted in hospital inpatient departments, and the typical treatment duration ranged from 1 to 2 weeks. Compared with conventional Western medicine alone, acupuncture combined with conventional Western medicine showed greater effectiveness (RR = 1.23, 95%CI 1.17 ~ 1.29, p < 0.001). Acupuncture significantly improved lung function (FEV1%: MD = 5.67, 95%CI 2.97 ~ 8.37, p < 0.001; FEV1/FVC: MD = 4.44, 95%CI 1.86 ~ 7.03, p < 0.001; FEV1: MD = 0.37, 95%CI 0.26 ~ 0.47, p < 0.001), reduced hypoxia (PaO2: MD = 3.60, 95%CI 2.23 ~ 4.98, p < 0.001; PaCO2: MD = -3.30, 95%CI -5.80 ~ -0.80, p < 0.05; SaO2: MD = 4.23, 95%CI 3.02 ~ 5.43, p < 0.001), and improved exercise tolerance (6MWT: MD = 40.34, 95%CI 30.50 ~ 50.17, p < 0.001), quality of life (CAT: MD = -2.68, 95%CI -3.39 ~ -1.96, p < 0.001), and dyspnea (mMRC: MD = -0.33, 95%CI -0.47 ~ -0.20, p < 0.001). However, the weaning success rate did not show a statistically significant difference between the two groups (RR = 1.18, 95%CI 0.95 ~ 1.48, p = 0.14). Mild side effects were reported in some studies. We rated the quality of evidence as very low to medium.
Conclusion: This systematic review and meta-analysis demonstrate that acupuncture, as an adjunctive treatment for acute exacerbations of chronic obstructive pulmonary disease, improves clinical efficacy and key outcomes. Our findings are consistent with previous studies that demonstrated improvements in the COPD Assessment Test (CAT) and arterial blood gas parameters (PaO2 and PaCO2). Unlike previous meta-analyses, the present study showed that adjunctive acupuncture significantly improved patient lung function FEV1% outcomes and significantly improved patient 6-min walk distance and modified Medical Research Council (mMRC) score; however, there was no significant difference in the success rate of weaning between the two groups. Although the review highlights clinical benefits, the heterogeneity of the included studies and the overall quality of the evidence suggest that more high-quality randomized controlled trials are needed to validate these findings and optimize treatment strategies. These studies should also prioritize standardizing acupuncture regimens, extending treatment duration, and conducting long-term follow-up assessments.
Systematic review registration: https://www.crd.york.ac.uk/prospero/ ID:CRD42024528155.
Keywords: acupuncture; acute exacerbation of chronic obstructive pulmonary disease; efficacy; meta-analysis; systematic review.
Copyright © 2025 Li, Liu, Yang, Li, He, Fei, Wei and Zhao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effects of external diaphragm pacing combined with conventional rehabilitation therapies in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis.Ther Adv Respir Dis. 2023 Jan-Dec;17:17534666231218086. doi: 10.1177/17534666231218086. Ther Adv Respir Dis. 2023. PMID: 38140896 Free PMC article.
-
Exploration of quantitative-effectiveness association between acupuncture temporal parameters and stable chronic obstructive pulmonary disease: A systematic review and dose-response meta-analysis of randomized controlled trials.Complement Ther Med. 2024 Jun;82:103048. doi: 10.1016/j.ctim.2024.103048. Epub 2024 May 10. Complement Ther Med. 2024. PMID: 38734186
-
Effects of Qingjin Huatan decoction on pulmonary function and inflammatory mediators in acute exacerbations of chronic obstructive pulmonary disease: a systematic review and meta-analysis.Front Pharmacol. 2024 Oct 18;15:1466677. doi: 10.3389/fphar.2024.1466677. eCollection 2024. Front Pharmacol. 2024. PMID: 39494348 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Optimal intensity and type of lower limb aerobic training for patients with chronic obstructive pulmonary disease: a systematic review and network meta-analysis of RCTs.Ther Adv Respir Dis. 2025 Jan-Dec;19:17534666251323190. doi: 10.1177/17534666251323190. Epub 2025 Mar 13. Ther Adv Respir Dis. 2025. PMID: 40083154 Free PMC article.
Cited by
-
Acupuncture for Chronic Obstructive Pulmonary Disease: A 38-Year Bibliometric Landscape of Global Research Trends and Knowledge Evolution (1986-2024).Int J Chron Obstruct Pulmon Dis. 2025 Jul 14;20:2393-2408. doi: 10.2147/COPD.S531611. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 40688235 Free PMC article.
-
Potential active ingredients and mechanisms of Shufeitie ointment in the treatment of chronic obstructive pulmonary disease by integrating transdermal chemistry and network pharmacology.Front Med (Lausanne). 2025 Jul 8;12:1605372. doi: 10.3389/fmed.2025.1605372. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40697927 Free PMC article.
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) . Global strategy for prevention, diagnosis and management of chronic obstructive pulmonary disease: 2025 report. (2024). Available online at: http://www.goldcopd.org/2025-gold-report/ (accessed November 11, 2024).
-
- Shah CH, Onukwugha E, Zafari Z, Villalonga-Olives E, Park JE, Slejko JF. Economic burden of comorbidities among COPD patients hospitalized for acute exacerbations: an analysis of a commercially insured population. Expert Rev Pharmacoecon Outcomes Res. (2022) 22:683–90. doi: 10.1080/14737167.2021.1981291, PMID: - DOI - PubMed
-
- Nordon C, Rhodes K, Quint JK, Vogelmeier CF, Simons SO, Hawkins NM, et al. . Exacerbations of Copd and their outcomes on cardiovascular diseases (Exacos-cv) Programme: protocol of multicountry observational cohort studies. BMJ Open. (2023) 13:e070022. doi: 10.1136/bmjopen-2022-070022, PMID: - DOI - PMC - PubMed
-
- Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. (2018) 198:464–71. doi: 10.1164/rccm.201710-2029OC, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous