

Preoperative submaximal cardiopulmonary exercise testing and its association with early postoperative complications
- PMID: 40421445
- PMCID: PMC12105740
- DOI: 10.1016/j.bjao.2025.100407
Preoperative submaximal cardiopulmonary exercise testing and its association with early postoperative complications
Abstract
Background: Early postoperative complication risk prediction would enhance perioperative surveillance and resource allocation. Reports have described brief submaximal cardiopulmonary exercise testing (CPET) for the routine assessment of cardiopulmonary disease. Compared with conventional CPET, it can be performed in 6 min and is used to predict peak CPET measurements. We aimed to determine whether submaximal CPET-derived measures outperform structured surveys in early postoperative complication detection.
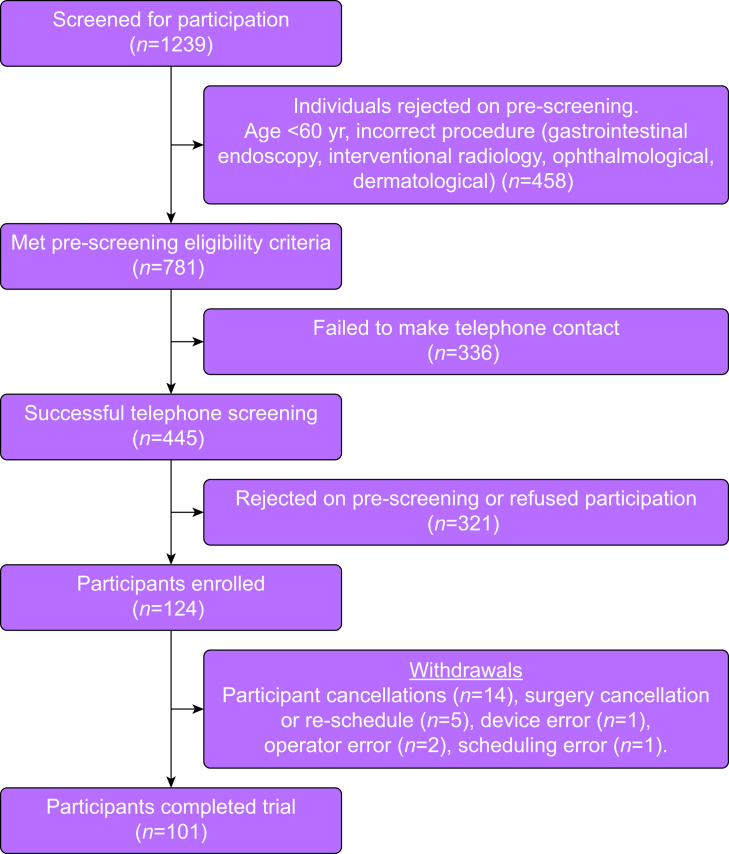
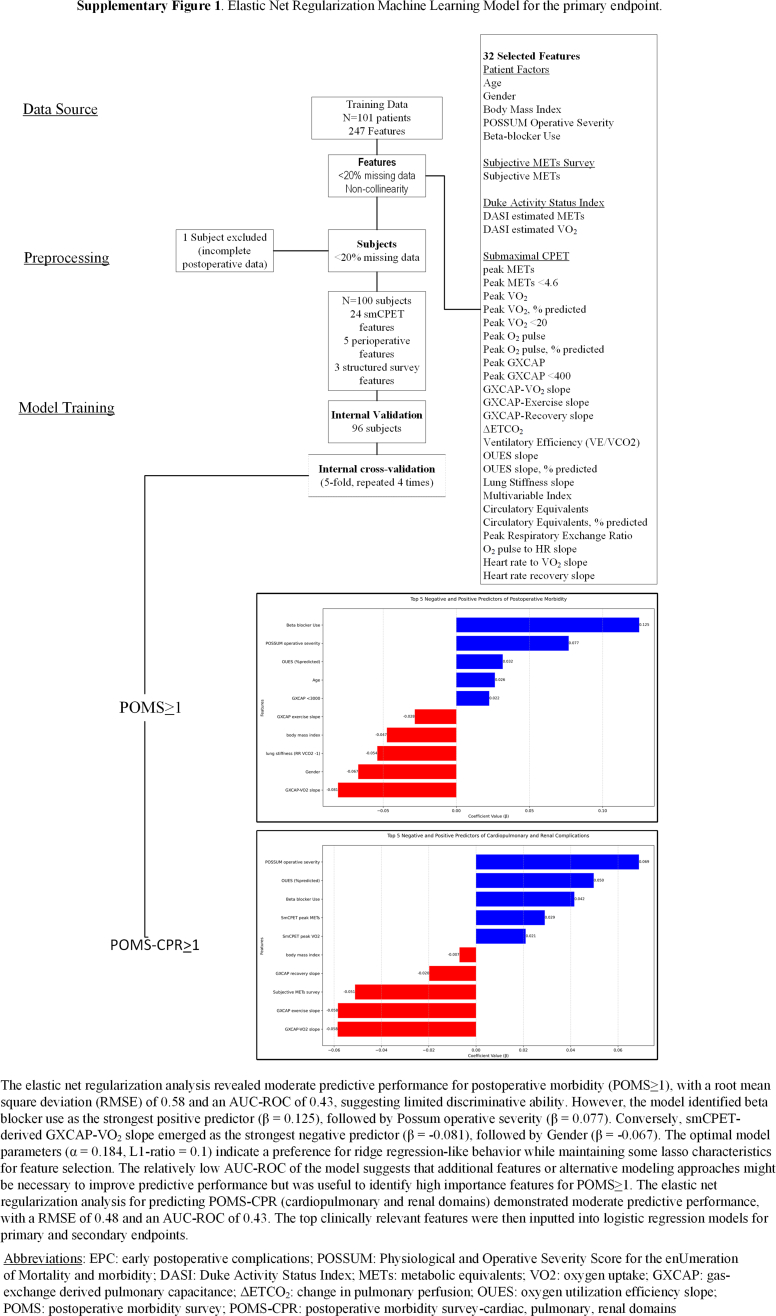
Methods: An institutional review board-approved, single-centre, open-label, clinical device trial was conducted. A total of 101 participants undergoing noncardiac surgery, aged >60 yr, with revised cardiac risk index ≤2, self-reported metabolic equivalents >4 (METs in ml O2 kg-1 min-1; self-endorsed reliably climbing two flights of stairs), were enrolled. Participants completed a subjective METs assessment, Duke Activity Status Index, and submaximal CPET that derived peak oxygen uptake (VO2, ml O2kg-1 min-1), METs, and gas exchange-derived pulmonary capacitance (GXCAP, in ml O2 beat-1 kPa-1). Elastic net regularisation machine learning identified feature importance among study measures for the primary endpoint (Postoperative Morbidity Survey [POMS] ≥1), secondary endpoints (cardiac, pulmonary and renal domains of the POMS [POMS-CPR ≥1]), and length of stay. Adjusted multivariable regression models were used to identify significance.
Results: Of 101 participants, 53 (52.4%) had POMS ≥1. GXCAP to peak VO2 slope (GXCAP-VO2) was associated with POMS ≥1 (ORadj 0.94; 95% CI 0.89-0.99; P=0.011) and increasing length of stay (ORadj 0.98; 95% CI 0.96-0.99; P=0.01). GXCAP-VO2 slope (ORadj 0.93; 95% CI 0.88-0.99; P=0.015) was associated with POMS-CPR ≥1.
Conclusions: Compared with structured surveys (subjective METs or Duke Activity Status Index) or conventional peak CPET values (VO2 or METs), a novel measure, GXCAP-VO2 slope, offered superior early postoperative complication discrimination in low-morbidity subjects. These preliminary findings support GXCAP-VO2 slope as a compelling investigational target for early postoperative complication risk, supporting the use of CPET to enhance early postoperative complication prediction.
Clinical trial registration: NCT05743673.
Keywords: early postoperative complications; preoperative evaluation; preoperative functional capacity; preoperative risk stratification; submaximal cardiopulmonary exercise testing.
© 2025 The Author(s).
Conflict of interest statement
ZJC declares partial research funding from Shape Medical Systems, Inc (MN, USA). PMH declares consulting for Cardiage LLC and Baudax Bio, consulting and sponsored research for Edwards Lifesciences, and equity interest in emka Medical.
Figures



References
-
- Stokes S.M., Scaife C.L., Brooke B.S., et al. Hospital costs following surgical complications: a value-driven outcomes analysis of cost savings due to complication prevention. Ann Surg. 2022;275:e375–e381. - PubMed
-
- Grocott M.P., Browne J.P., Van der Meulen J., et al. The Postoperative Morbidity Survey was validated and used to describe morbidity after major surgery. J Clin Epidemiol. 2007;60:919–928. - PubMed
-
- Lurati Buse G.A.L., Puelacher C., Gualandro D.M., et al. Association between self-reported functional capacity and major adverse cardiac events in patients at elevated risk undergoing noncardiac surgery: a prospective diagnostic cohort study. Br J Anaesth. 2021;126:102–110. - PubMed
-
- Fleisher L.A., Fleischmann K.E., Auerbach A.D., et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2014;64:e77–e137. - PubMed
-
- Reilly D.F., McNeely M.J., Doerner D., et al. Self-reported exercise tolerance and the risk of serious perioperative complications. Arch Intern Med. 1999;159:2185–2192. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
