

Trading off Iodine and Radiation Dose in Coronary Computed Tomography
- PMID: 40422966
- PMCID: PMC12112519
- DOI: 10.3390/jcdd12050195
Trading off Iodine and Radiation Dose in Coronary Computed Tomography
Abstract
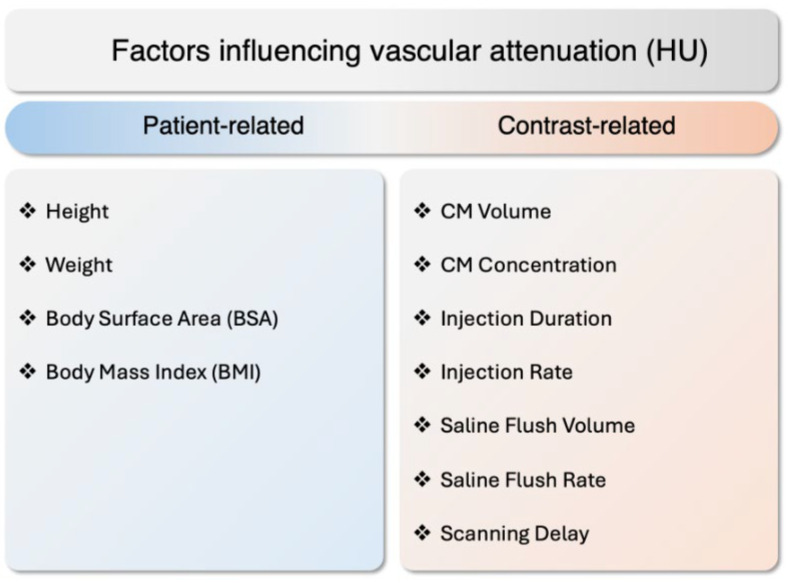
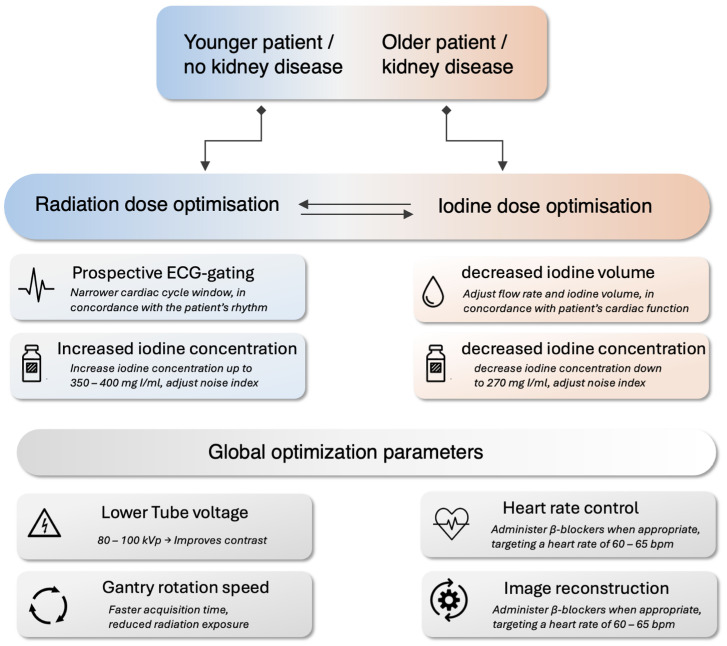
Coronary CT angiography (CCTA) has seen steady progress since its inception, becoming a key player in the non-invasive assessment of coronary artery disease (CAD). Advancements in CT technology, including iterative and deep-learning-based reconstruction, wide-area detectors, and dual-source systems, have helped mitigate early limitations, such as high radiation doses, motion artifacts, high iodine load, and non-diagnostic image quality. However, the adjustments between ionizing radiation and iodinated contrast material (CM) volumes remain a critical concern, especially due to the increasing use of CCTA in various indications. This review explores the balance between radiation and CM volumes, emphasizing patient-specific protocol optimization to improve diagnostic accuracy while minimizing risks. Radiation dose reduction strategies, such as low tube voltage protocols, prospective ECG-gating, and modern reconstruction algorithms, have significantly decreased radiation exposure, with some studies achieving sub-millisievert doses. Similarly, CM volume optimization, including adjustments in strategies for calculating CM volume, iodine concentration, and flow protocols, plays a role in managing risks such as contrast-associated acute kidney injury, particularly in patients with renal impairment. Emerging technologies, such as photon-counting CT and deep-learning reconstruction, promise further improvements in dose efficiency and image quality. This review summarizes current evidence, highlights the benefits and limitations of dose control approaches, and provides practical recommendations for practitioners. By tailoring protocols to patient characteristics, such as age, renal function, and body habitus, clinicians can achieve an optimal trade-off between diagnostic accuracy and patient safety, ensuring optimal operation of CT systems in clinical practice.
Keywords: contrast-induced acute kidney injury; coronary CT angiography; coronary artery disease; iodinated contrast media; patient-specific protocols; radiation dosage.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Coronary CT angiography with 80 kV tube voltage and low iodine concentration contrast agent in patients with low body weight.J Cardiovasc Comput Tomogr. 2016 Jul-Aug;10(4):322-6. doi: 10.1016/j.jcct.2016.06.003. Epub 2016 Jun 15. J Cardiovasc Comput Tomogr. 2016. PMID: 27357327
-
Effect of reduced x-ray tube voltage, low iodine concentration contrast medium, and sinogram-affirmed iterative reconstruction on image quality and radiation dose at coronary CT angiography: results of the prospective multicenter REALISE trial.J Cardiovasc Comput Tomogr. 2015 May-Jun;9(3):215-24. doi: 10.1016/j.jcct.2015.01.010. Epub 2015 Jan 22. J Cardiovasc Comput Tomogr. 2015. PMID: 25843243 Clinical Trial.
-
Reducing both radiation and contrast doses in coronary CT angiography in lean patients on a 16-cm wide-detector CT using 70 kVp and ASiR-V algorithm, in comparison with the conventional 100-kVp protocol.Eur Radiol. 2019 Jun;29(6):3036-3043. doi: 10.1007/s00330-018-5837-9. Epub 2018 Nov 30. Eur Radiol. 2019. PMID: 30506217
-
Low-Dose Radiation Advances in Coronary Computed Tomography Angiography in the Diagnosis of Coronary Artery Disease.Curr Cardiol Rev. 2019;15(4):304-315. doi: 10.2174/1573403X15666190222163737. Curr Cardiol Rev. 2019. PMID: 30806322 Free PMC article. Review.
-
Did low tube voltage CT combined with low contrast media burden protocols accomplish the goal of "double low" for patients? An overview of applications in vessels and abdominal parenchymal organs over the past 5 years.Int J Clin Pract. 2016 Sep;70 Suppl 9B:B5-B15. doi: 10.1111/ijcp.12861. Int J Clin Pract. 2016. PMID: 27577514 Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
