

A multi-center retrospective analysis of ultrasound-guided fine needle aspiration biopsy for detecting additional positive axillary node metastasis in early breast cancer
- PMID: 40425612
- PMCID: PMC12116892
- DOI: 10.1038/s41598-025-01353-z
A multi-center retrospective analysis of ultrasound-guided fine needle aspiration biopsy for detecting additional positive axillary node metastasis in early breast cancer
Abstract
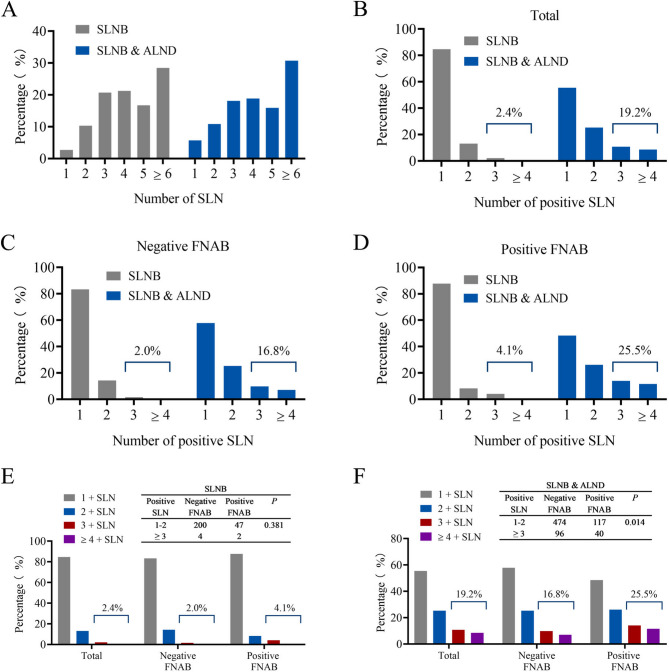
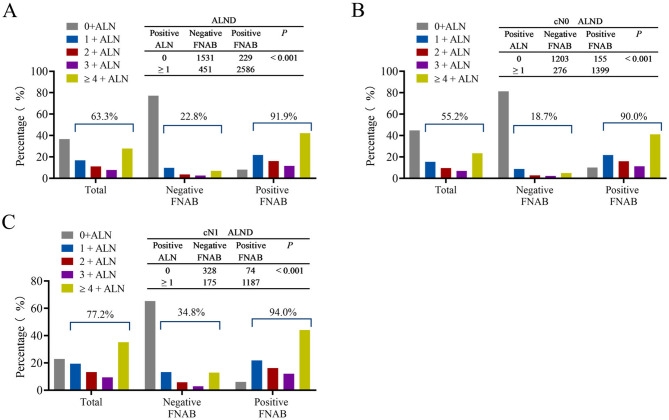
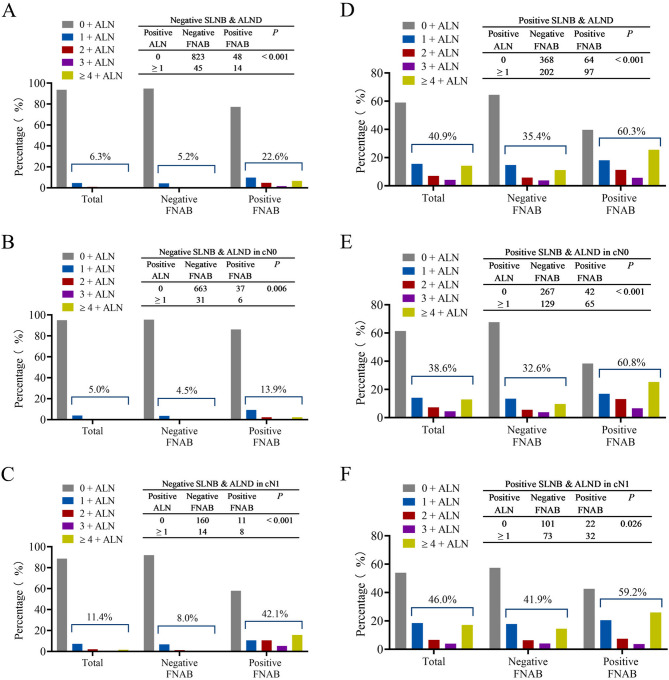
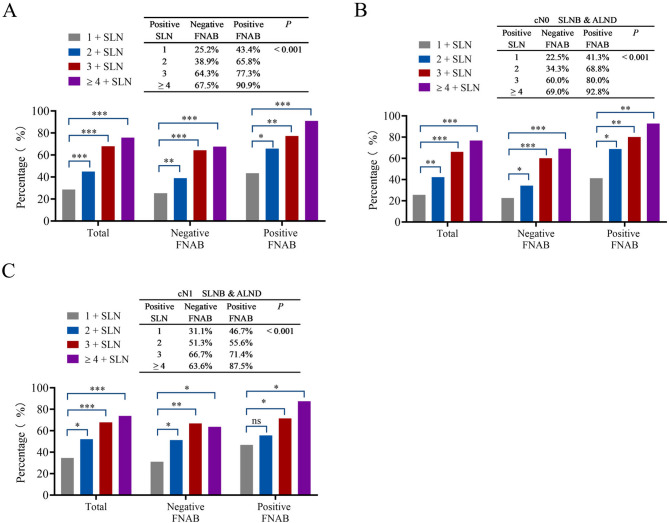
This study evaluates the effectiveness of ultrasound-guided fine needle aspiration biopsy (US-FNAB) in assessing additional positive axillary lymph node (ALN) metastasis following sentinel lymph node biopsy (SLNB) in clinically ALN-negative or N1 cases, aiming to refine patient management. A multi-center, retrospective analysis included 7617 patients with cT1-2 and cN0-1, who underwent US-FNAB for ALN and proceeding to SLNB or axillary lymph node dissection (ALND). Metastatic patterns were assessed, particularly focusing on correlations with positive FNAB results and additional ALN metastasis found during ALND, with statistical significance evaluated. Of those undergoing SLNB, 97.5% exhibited macrometastasis. In the SLNB-only group, 2.4% had 3 and more than 3 positive lymph node, compared to 19.2% in the SLNB & ALND group (P < 0.01). Among ALND patients, 63.3% had positive nodes, significantly higher in those with positive FNAB (91.9% vs. 22.8%, P < 0.001). Additionally, 40.9% were found to have additional positive ALNs in patients who underwent ALND following positive SLNB, with rates significantly higher in those with positive FNAB (60.3% vs. 35.4%, P < 0.001). LVI positivity, pT2-3, SLNR > 50% and positive FNAB were independent predictors of additional ALN metastasis in patients undergoing ALND after positive SLNB (P < 0.05). The proportion of additional positivity escalated with the number of positive SLNs. US-FNAB significantly improves the detection of additional ALN metastasis, guiding more effective strategy for ALN surgical decision-making. Our findings support the incorporation of US-FNAB into clinical practice to improve patient stratification and optimize treatment outcomes in early-stage breast cancer management.
Keywords: Axillary lymph node dissection; Early breast cancer; Fine needle aspiration biopsy; Sentinel lymph node biopsy; Ultrasound-guided.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bryan, R. M., Mercer, R. J., Bennett, R. C. & Rennie, G. C. Prognostic factors in breast cancer and the development of a prognostic index. J. Br. Surg.73, 267–271 (1986). - PubMed
-
- Goyal, A., Newcombe, R. G., Chhabra, A. & Mansel, R. E. Morbidity in breast Cancer patients with Sentinel node metastases undergoing delayed axillary lymph node dissection (ALND) compared with immediate ALND. Ann. Surg. Oncol.15, 262–267 (2007). - PubMed
-
- Fraile, M. et al. Julián Fj Fau - Fusté F, Llatjós M Fau - Castellà E,. Sentinel node biopsy as a practical alternative to axillary lymph node dissection in breast cancer patients: an approach to its validity. Annals of Oncology. ; 11: 701-5. (2000). - PubMed
-
- Purushotham, A. D. et al. Fau - Myles JP, Myles Jp Fau - Duffy SW,. Morbidity after sentinel lymph node biopsy in primary breast cancer: results from a randomized controlled trial. Journal of Clinical Oncology. ; 23: 4312-21. (2005). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
