

Postpartum administration of eplerenone to mitigate vascular dysfunction in mice following a preeclampsia-like pregnancy
- PMID: 40425613
- PMCID: PMC12116800
- DOI: 10.1038/s41598-025-02475-0
Postpartum administration of eplerenone to mitigate vascular dysfunction in mice following a preeclampsia-like pregnancy
Abstract
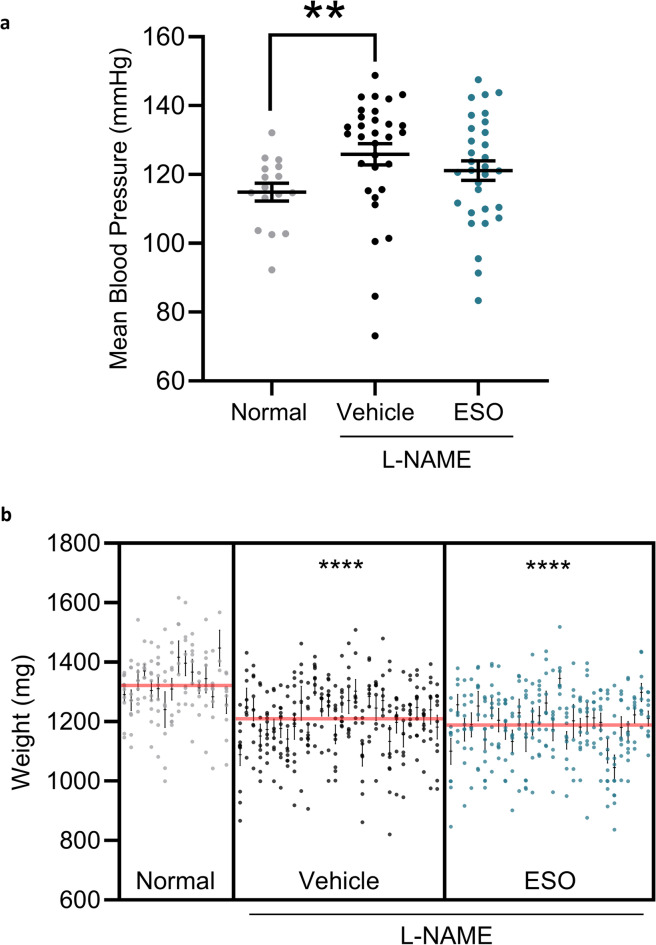
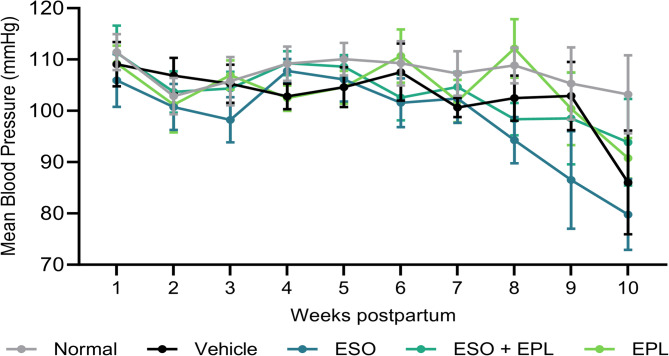
Preeclampsia is a severe pregnancy complication associated with substantial injury to systemic vasculature, major organs, and the feto-placental unit, with an approximate mortality rate of 76,000 pregnant women and 500,000 babies each year. Preeclampsia results in up to five-fold increased risk of cardiovascular disease. There is currently no cure and limited treatment options for preeclampsia and its long-term effects. In this study, we modelled preeclampsia in the mouse via nitric oxide blockade and examined the effect of therapeutic intervention during pregnancy (esomeprazole) and postpartum (eplerenone) on indices of cardiovascular health. Pregnant CBA x C57BL/6 mice received 50 mg/kg/day N(ω)-nitro-L-arginine methyl ester to induce a preeclampsia-like phenotype. Mice were treated with either 12.5 mg/kg/day esomeprazole during pregnancy, 55.5 mg/kg/day eplerenone during the postpartum period, or both esomeprazole and eplerenone in sequence. Mice were hypertensive during pregnancy, fetal growth was restricted by 10%, and maternal vasoactivity was impaired at 5-weeks postpartum. Eplerenone treatment (± esomeprazole) reduced vasoconstriction at 5-weeks postpartum and enhanced vasorelaxation at 5- and 10-weeks postpartum, supporting improved cardiovascular indices in the medium to long term postpartum period. Postpartum eplerenone treatment may be beneficial in mitigating consequent cardiovascular disease risk following a pregnancy complicated by preeclampsia.
Keywords: Cardiovascular disease; Eplerenone; L-NAME; Mouse model; Preeclampsia; Pregnancy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures



References
-
- Duley, L. The global impact of pre-eclampsia and eclampsia. Semin. Perinatol.33, 130–137. 10.1053/j.semperi.2009.02.010 (2009). - PubMed
-
- Kuklina, E. V., Ayala, C. & Callaghan, W. M. Hypertensive disorders and severe obstetric morbidity in the united States. Obstet. Gynecol.113, 1299–1306. 10.1097/AOG.0b013e3181a45b25 (2009). - PubMed
-
- Paruk, F. & Moodley, J. Maternal and neonatal outcome in early- and late-onset pre-eclampsia. Semin. Neonatol. 5, 197–207. 10.1053/siny.2000.0023 (2000). - PubMed
-
- Venkatesha, S. et al. Soluble endoglin contributes to the pathogenesis of preeclampsia. Nat. Med.12, 642–649. 10.1038/nm1429 (2006). - PubMed
MeSH terms
Substances
Grants and funding
- seed funding/Baker Department of Cardiometabolic Health
- seed funding/Baker Department of Cardiometabolic Health
- Baker Trust Alice Baker and Eleanor Shaw Gender Equity Fellowship/Diabetes Australia
- Operational Infrastructure Scheme/State Government of Victoria
- 1146128/National Health and Medical Research Council
LinkOut - more resources
Full Text Sources
