

Correlation between Tomographic and Histopathological Staging in Upfront Resected Gastric Cancer: Enhancing Diagnostic Accuracy in the Era of Perioperative Therapy
- PMID: 40425902
- PMCID: PMC12116807
- DOI: 10.1007/s12029-025-01245-5
Correlation between Tomographic and Histopathological Staging in Upfront Resected Gastric Cancer: Enhancing Diagnostic Accuracy in the Era of Perioperative Therapy
Abstract
Purpose: This study aimed to assess the diagnostic accuracy of multidetector contrast-enhanced computerised tomography (MDCT) and to establish a correlation between radiological and histopathological staging in upfront resected localised gastric cancers (GC).
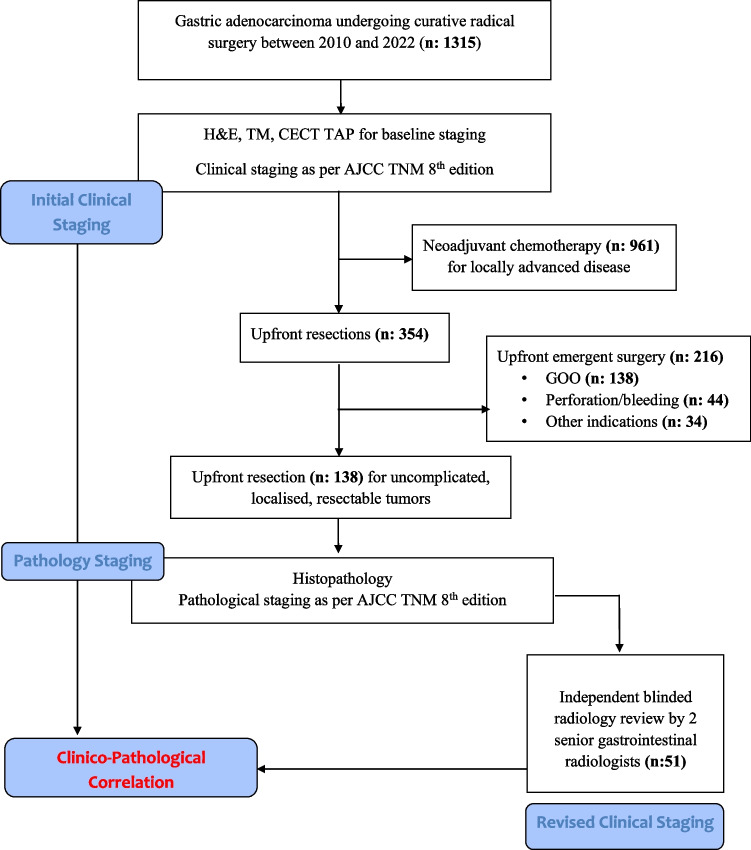
Methods: All consecutive patients of resectable, localised GC who underwent upfront elective resection between 2010 and 2022 were included. The initial clinical staging determined during multidisciplinary meetings was compared with the pathological stage obtained after surgery. Subsequently, a retrospective, blinded review was conducted to assign a revised clinical staging, and accuracy was correlated.
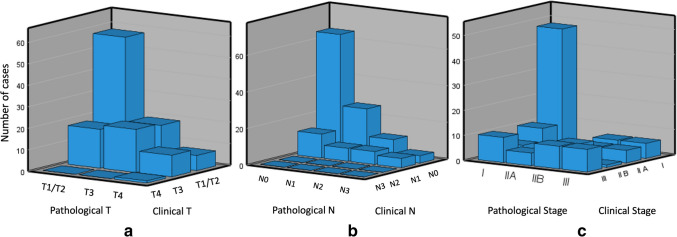
Results: The analysis of 138 patients revealed varying accuracy of MDCT in determining the T stage (66.9% for T1/T2, 64.6% for T3, and 87.2% for T4) and N stage (60.8% for N0, 63.7% for N1, and 83.2% for N2). The accuracy for stage group ranged from 71 to 78.65%. There was weak agreement observed between the T, N, and overall stage on clinicopathological correlation. However, a blinded radiology review by oncoradiologists resulted in improved accuracy, particularly in T1/T2 disease, and also improved pathological stage correlation.
Conclusions: Although MDCT is a valuable initial staging tool for gastric cancer, we found weak agreement between the clinical and the pathological stages in upfront resected gastric cancers. By implementing an expert radiology review and standardising scanning and reporting protocols, we can significantly improve the accuracy and correlation of MDCT with pathology, even for T1/T2 disease. This may help in better selecting patients for upfront surgery versus perioperative chemotherapy, especially in resource-constrained settings.
Keywords: Computerised tomography; Correlation; Gastric cancer; Histopathology; Upfront resection.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics Approval and Consent to Participate: The data of the present study were collected in the course of common clinical practice, and accordingly, the signed informed consent was obtained from each patient for any surgical and clinical procedure. The study protocol was in accordance with the ethical standards of the institutional research committee and the 1964 Helsinki Declaration and its later amendments. Consent for Publication: Data was collected retrospectively, and all reasonable measures were taken to protect patient anonymity. Competing Interests: The authors declare no competing interests.
Figures
References
-
- Hamashima C, Systematic Review Group and Guideline Development Group for Gastric Cancer Screening Guidelines. Update version of the Japanese guidelines for gastric cancer screening. Japanese journal of clinical oncology. 2018;48(7):673–83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous