

Assessment of surgical capacity and productivity in high-volume Ethiopian hospitals: mixed method study
- PMID: 40426140
- PMCID: PMC12107986
- DOI: 10.1186/s12913-025-12892-6
Assessment of surgical capacity and productivity in high-volume Ethiopian hospitals: mixed method study
Abstract
Background: In Ethiopia and other low-and middle-income countries, access to emergency and elective surgical care is still inadequate and inequitable. Ethiopia has initiated a nationwide strategic plan aimed at tackling obstacles within the surgical system. The aim of this study was to assess surgical and anesthesia care capacity and productivity in high volume Ethiopian hospitals.
Methods: An explanatory mixed-methods study was conducted in 24 high-volume public hospitals across Ethiopia's 10 regions and 2 city administrations. Data were collected through structured document reviews, site observations, and interviews using a validated WHO-aligned tool. Quantitative data were analyzed using SPSS, and qualitative responses were thematically analyzed using ATLAS.ti.
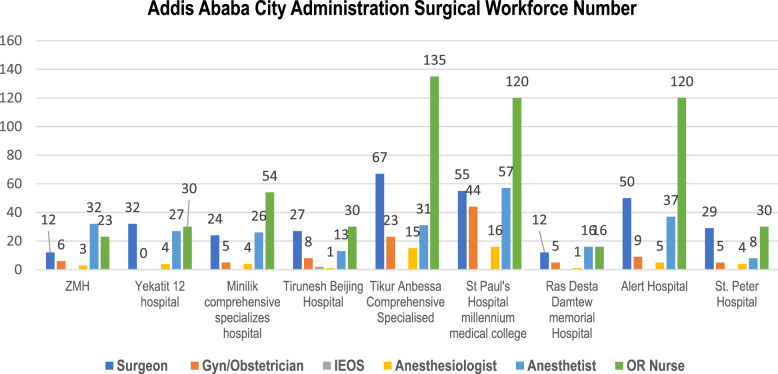
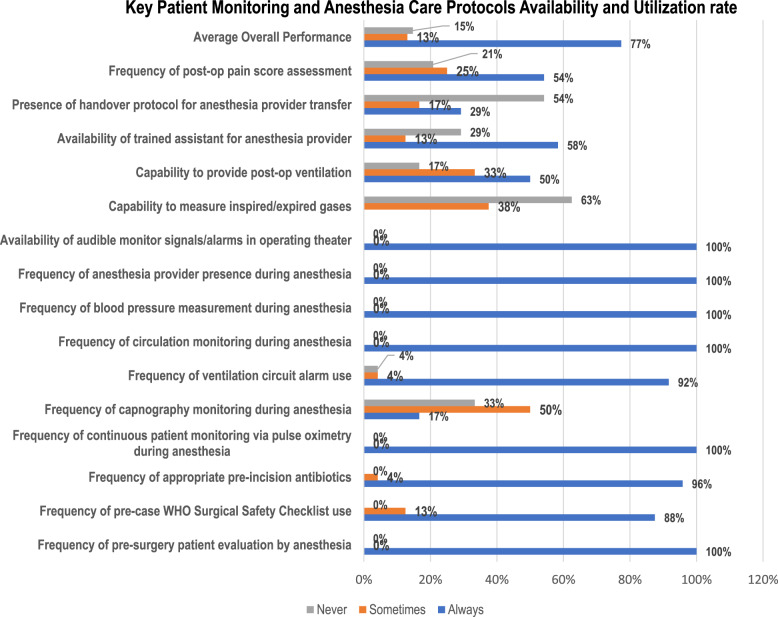
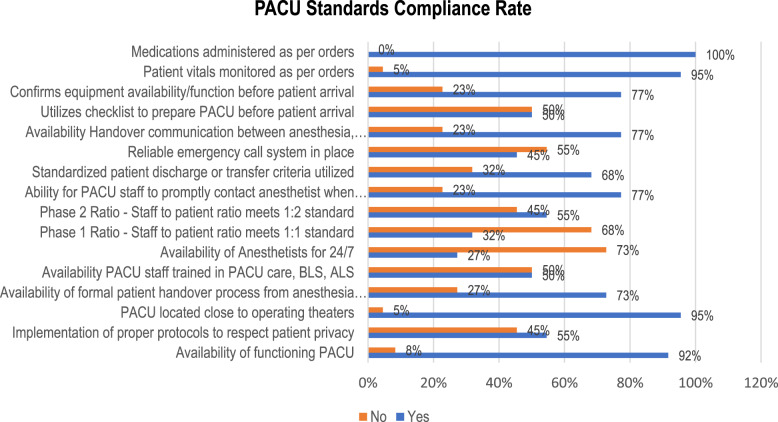
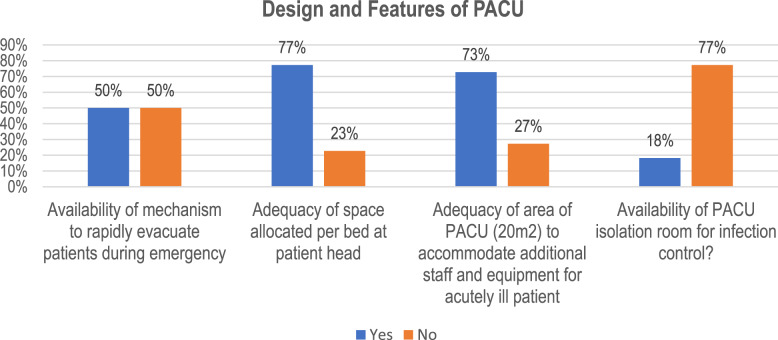
Results: Addis Ababa hosts over 60% of the national surgical workforce, highlighting stark regional disparities. While 80% of hospitals reported adequate infrastructure, site observations revealed functional inconsistencies in PACU design, sterilization units, and equipment availability. Only 77% of hospitals consistently implemented patient monitoring and handover protocols. Surgical productivity was low, with an average of 2.5 surgeries per week per clinician and 52.39% annual workforce productivity. Best practices included the use of EMRs, backlog-reduction campaigns, and daily interdisciplinary briefings. However, persistent challenges included inadequate staffing, poor infrastructure, and uneven adoption of safety protocols.
Conclusion and recommendation: Ethiopia's surgical system shows promising innovations in select hospitals, yet national scale-up is hindered by infrastructure gaps, uneven workforce distribution, and inconsistent safety practices. Addressing these challenges requires data-driven planning, targeted investment in underserved regions, and expanded use of digital systems and collaborative networks to promote best practice adoption across facilities.
Keywords: Ethiopia; Infrastructure; Productivity; Surgical and anesthesia workforce.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for this study was obtained from the Ethiopian Association of Anesthetists Institutional Research Ethics Review Committee (Protocol number: /0895/007/2016). Informed consent was obtained from all participants prior to their participation. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.16/3 Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
Medical doctors profile in Ethiopia: production, attrition and retention. In memory of 100-years Ethiopian modern medicine & the new Ethiopian millennium.Ethiop Med J. 2008 Jan;46 Suppl 1:1-77. Ethiop Med J. 2008. PMID: 18709707
-
Mixed-methods assessment of surgical capacity in two regions in Ethiopia.Br J Surg. 2019 Jan;106(2):e81-e90. doi: 10.1002/bjs.11032. Br J Surg. 2019. PMID: 30620064
-
Trauma team members' perceptions of the effectiveness of the current trauma care system in Addis Ababa, Ethiopia: a phenomenological study.BMC Health Serv Res. 2025 Mar 31;25(1):472. doi: 10.1186/s12913-025-12611-1. BMC Health Serv Res. 2025. PMID: 40165192 Free PMC article.
-
Assessing Ethiopia's surgical capacity in light of global surgery 2030 initiatives: Is there progress in the past decade?Surg Open Sci. 2024 Mar 28;19:70-79. doi: 10.1016/j.sopen.2024.03.015. eCollection 2024 Jun. Surg Open Sci. 2024. PMID: 38595832 Free PMC article. Review.
-
The Status of Facility Based Emergency Care in Public Hospitals of Ethiopia Using WHO Assessment Tool.Ethiop J Health Sci. 2022 Nov;32(6):1093-1100. doi: 10.4314/ejhs.v32i6.5. Ethiop J Health Sci. 2022. PMID: 36475266 Free PMC article.
Cited by
-
Unfavorable management outcome and its predictors among appendicitis patients in ethiopia: a systematic review and meta- analysis.BMC Surg. 2025 Aug 9;25(1):354. doi: 10.1186/s12893-025-03108-z. BMC Surg. 2025. PMID: 40783541 Free PMC article.
References
-
- Bendix P, Havens JM. The global burden of surgical disease. Curr Trauma Rep. 2017;3(1):25–31.
-
- Shrime MG, Bickler SW, Alkire BC, Mock C. Global burden of surgical disease: an Estimation from the provider perspective. Lancet Global Health. 2015;3:S8–9. - PubMed
-
- Kurlberg G, Lancet Commission on Global Surgery - A Public Health Initiative. J Inst Med. 2020;42(1). Available from: https://www.nepjol.info/index.php/JIOM/article/view/37413. [cited 2024 Sep 14].
-
- Henker R, Taki M. Challenges to Global Access to Anesthesia and Surgical Care. In: Thomas SL, Rowles JS, editors. Nurse Practitioners and Nurse Anesthetists: The Evolution of the Global Roles. Cham: Springer International Publishing; 2023. pp. 313–29. (Advanced Practice in Nursing). Available from: https://link.springer.com/10.1007/978-3-031-20762-4_25. [cited 2025 Apr 8]. - DOI
-
- Blake C, Alkire, Alkire BC, Abebe Bekele, Bekele A, Isabelle Citron, Citron I, et al. Building capacity for surgery, obstetrics and anesthesia in support of universal health coverage and achievement of the sustainable development goals. East Cent Afr J Surg. 2019;24(1):3–8.
MeSH terms
Grants and funding
- 72066320CA00008/Ministry of Health, Ethiopia and USAID Health Workforce Improvement Program
- 72066320CA00008/Ministry of Health, Ethiopia and USAID Health Workforce Improvement Program
- 72066320CA00008/Ministry of Health, Ethiopia and USAID Health Workforce Improvement Program
- 72066320CA00008/Ministry of Health, Ethiopia and USAID Health Workforce Improvement Program
- 72066320CA00008/Ministry of Health, Ethiopia and USAID Health Workforce Improvement Program
LinkOut - more resources
Full Text Sources
