

Clinical and economic effectiveness of Schroth therapy in adolescent idiopathic scoliosis: insights from a machine learning- and active learning-based real-world study
- PMID: 40426247
- PMCID: PMC12117940
- DOI: 10.1186/s13018-025-05900-2
Clinical and economic effectiveness of Schroth therapy in adolescent idiopathic scoliosis: insights from a machine learning- and active learning-based real-world study
Abstract
Background: Adolescent idiopathic scoliosis (AIS) is a prevalent musculoskeletal condition affecting approximately 2-3% of the adolescent population. Although exercise-based therapeutic interventions are increasingly employed as non-surgical alternatives, their clinical and economic effectiveness remains underexplored in real-world settings. Recent advancements in active learning (AL) and machine learning (ML) techniques offer the potential to optimize treatment protocols by uncovering hidden predictors and enhancing model efficiency.
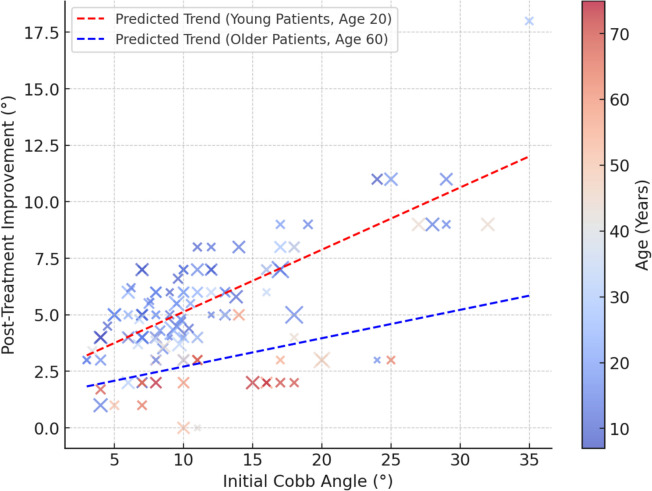
Methods: This retrospective study evaluated the clinical and cost-effectiveness of exercise-based therapy in 128 AIS patients treated between 2020 and 2023 at a tertiary public hospital. Patients were followed for 3 to 36 months. Clinical outcomes were assessed based on changes in Cobb angle, Visual Analogue Scale (VAS) scores for pain, and SRS-22r functional outcomes. Direct medical costs were extracted from institutional records to estimate the incremental cost-effectiveness ratio (ICER) and quality-adjusted life years (QALYs). In parallel, ML models, including Random Forest regression and AL strategies, were applied to predict treatment outcomes and enhance data labeling efficiency.
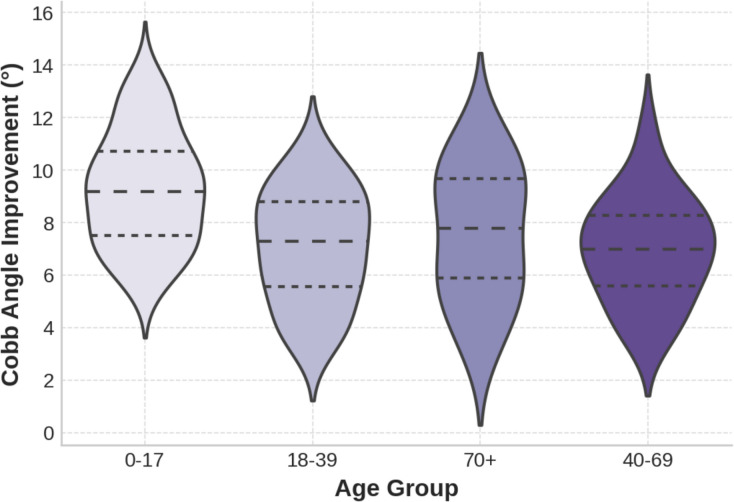
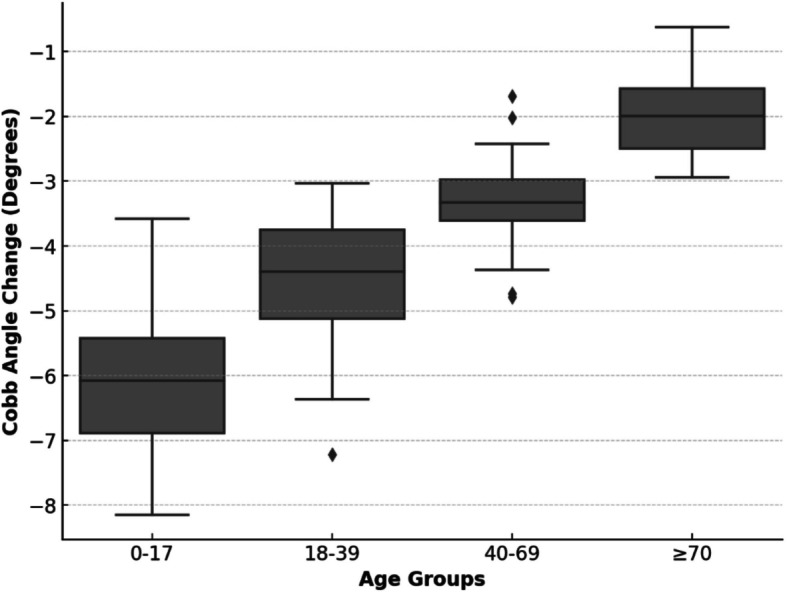
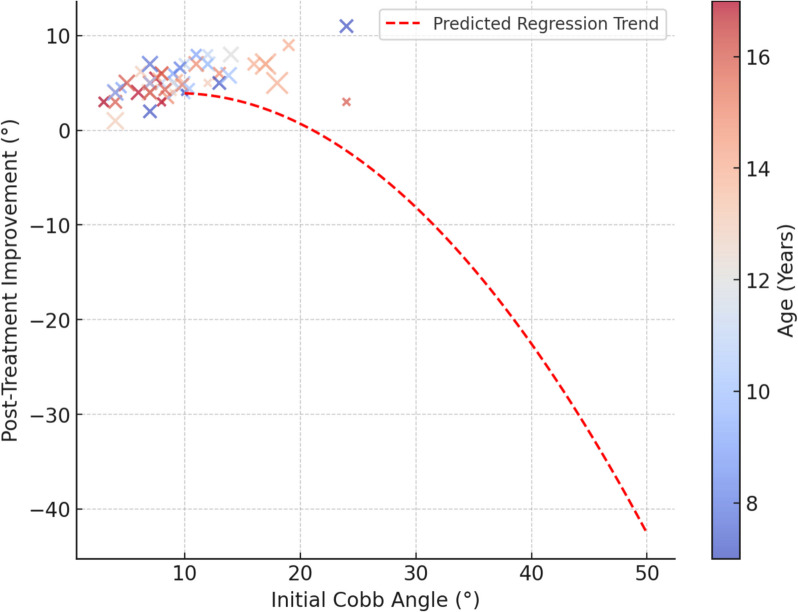
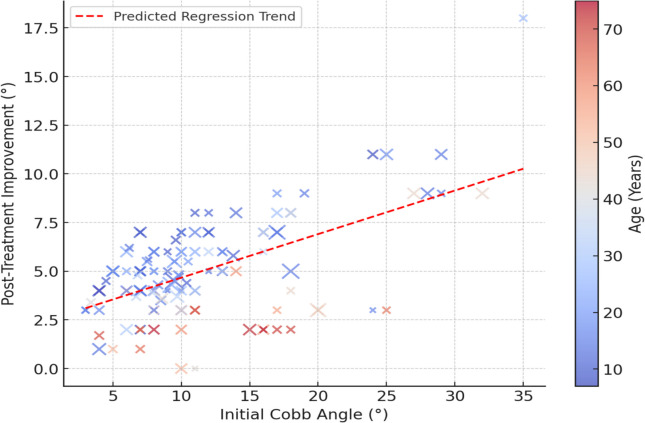
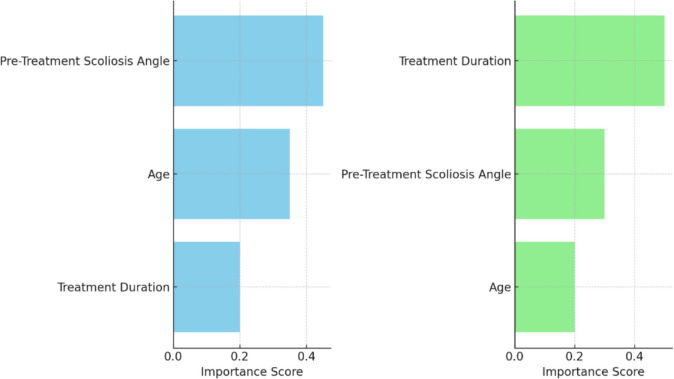
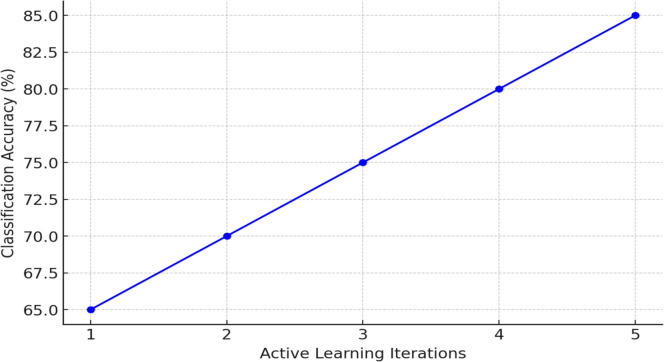
Results: Exercise-based therapy resulted in a mean Cobb angle reduction of 6.8° (SD = 3.1), with significant improvements in pain and function (p < 0.001). The ICER was estimated at $1,730 per additional degree of Cobb angle correction, with a projected QALY gain of 0.03 per patient. While treatment duration was statistically non-significant in traditional regression analyses (p > 0.1), ML models identified it as a top predictor of both Cobb angle correction and pain reduction. The Random Forest model achieved an MAE of 0.84 and an RMSE of 1.06 for pain reduction predictions, while AL improved classification accuracy from 65 to 85% across five iterations by selectively labeling the most uncertain cases. Sensitivity analyses confirmed the robustness of economic findings.
Conclusion: Exercise-based therapy, combined with ML and AL techniques, appears to be a clinically effective and economically sustainable intervention for AIS management. ML models identified important predictors overlooked by classical methods, particularly highlighting the importance of treatment duration. These findings may inform evidence-based strategies for integrating personalized, data-driven approaches into conservative scoliosis treatment protocols and optimizing musculoskeletal healthcare resource allocation.
Keywords: Active learning; Adolescent idiopathic scoliosis; Cost-effectiveness; Machine learning; Non-surgical treatment; Pain reduction; Schroth therapy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the İstanbul Esenyurt University Ethics Committee (Approval No: 2024–02, Date: 05.03.2024) in compliance with the principles of the Declaration of Helsinki and its latest amendments. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Patients with adolescent idiopathic scoliosis perceive positive improvements regardless of change in the Cobb angle - Results from a randomized controlled trial comparing a 6-month Schroth intervention added to standard care and standard care alone. SOSORT 2018 Award winner.BMC Musculoskelet Disord. 2019 Jul 8;20(1):319. doi: 10.1186/s12891-019-2695-9. BMC Musculoskelet Disord. 2019. PMID: 31286903 Free PMC article. Clinical Trial.
-
Effects of a Long-Term Supervised Schroth Exercise Program on the Severity of Scoliosis and Quality of Life in Individuals with Adolescent Idiopathic Scoliosis: A Randomized Clinical Trial Study.Medicina (Kaunas). 2024 Oct 7;60(10):1637. doi: 10.3390/medicina60101637. Medicina (Kaunas). 2024. PMID: 39459424 Free PMC article. Clinical Trial.
-
Schroth exercises improve health-related quality of life and radiographic parameters in adolescent idiopathic scoliosis patients.Chin Med J (Engl). 2021 Oct 13;134(21):2589-2596. doi: 10.1097/CM9.0000000000001799. Chin Med J (Engl). 2021. PMID: 34653079 Free PMC article.
-
The effectiveness of Schroth method in Cobb angle, quality of life and trunk rotation angle in adolescent idiopathic scoliosis: a systematic review and meta-analysis.Eur J Phys Rehabil Med. 2023 Apr;59(2):228-236. doi: 10.23736/S1973-9087.23.07654-2. Epub 2023 Jan 24. Eur J Phys Rehabil Med. 2023. PMID: 36692412 Free PMC article.
-
Evaluating exercise therapies in adolescent idiopathic scoliosis: a systematic review with Bayesian network meta-analysis.PeerJ. 2025 Mar 31;13:e19175. doi: 10.7717/peerj.19175. eCollection 2025. PeerJ. 2025. PMID: 40183057 Free PMC article.
References
-
- Yi J, Li M, Dong A, Luo YY, Luo CL, Zheng Q, Wang S, Wong MS, Ma CZH, Zhang M. Comparison between a state-of-the-art mechanical 3D scoliosis correction protocol and the Schroth exercise on spinal flexibility of patients with adolescent idiopathic scoliosis: A randomized controlled trial. Arch Rehabil Res Clin Transl. 2025;5(1):100428. 10.1016/j.arrct.2025.100428.
-
- de Vries A, de Boer T, van der Velde D. A systematic review on the impact of scoliosis on health-related quality of life. Eur Spine J. 2019;28(4):685–704. 10.1007/s00586-019-06135-5.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
