

Factors Predicting Myocardial Recovery After Hospitalization for De Novo Heart Failure with Reduced Left Ventricular Ejection Fraction: Results from the COMFE Registry
- PMID: 40426969
- PMCID: PMC12109323
- DOI: 10.3390/biomedicines13051143
Factors Predicting Myocardial Recovery After Hospitalization for De Novo Heart Failure with Reduced Left Ventricular Ejection Fraction: Results from the COMFE Registry
Abstract
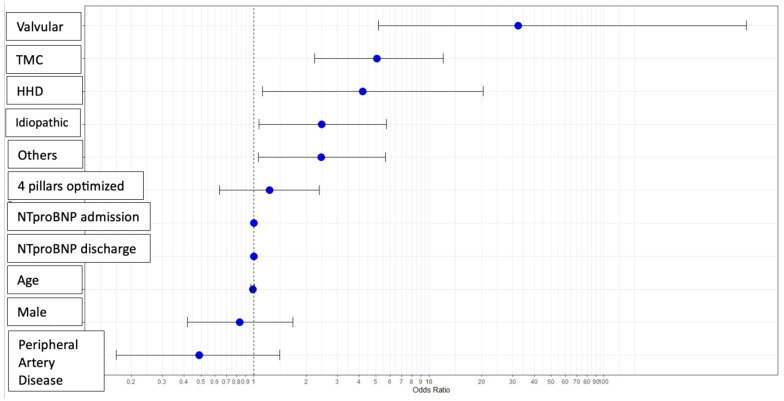
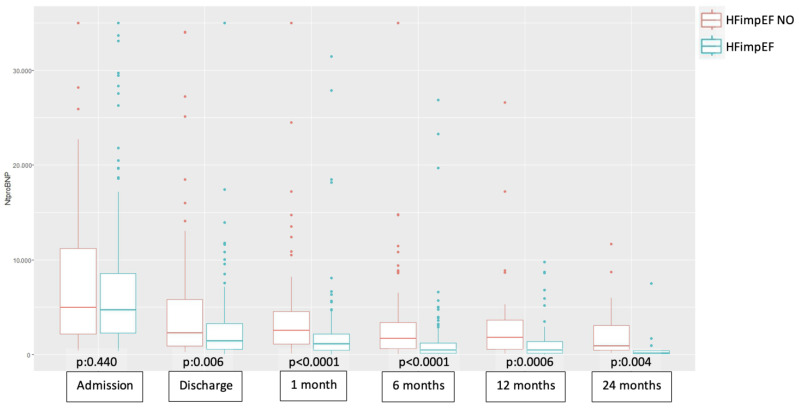
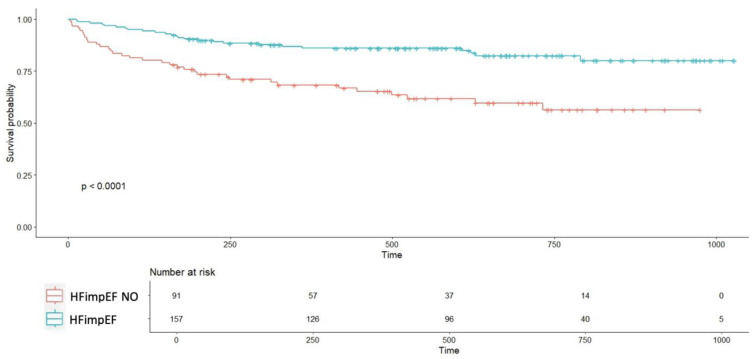
Background/Objectives: Patients hospitalized for de novo heart failure with reduced ejection fraction (HFrEF) may experience improvement in left ventricular function, a phenomenon associated with improved morbidity and mortality outcomes. However, the factors influencing this improvement remain unclear. This study aimed to investigate the association between clinical and therapeutic factors and short-term improvement or recovery of left ventricular ejection fraction (LVEF) in patients hospitalized with newly diagnosed heart failure with reduced ejection fraction (HFrEF). Methods: This was a prospective observational study conducted in two referral centers in Spain. All patients admitted with de novo HFrEF between March 2021 and December 2023 were included. Improved myocardial function (HFimpEF) was defined as an initial LVEF ≤ 40% and a follow-up echocardiogram showing LVEF > 40%, with an increase of ≥10 points from baseline. Results: In total, 157 patients (63.3%) met the criteria for HFimpEF. Among the various etiologies of heart failure, significant differences were found between groups for tachycardiomyopathy (HFimpEF: 29.3% vs. non-HFimpEF: 13.1%, p = 0.006), valvular (HFimpEF: 7.6% vs. non-HFimpEF: 1.1%, p = 0.05), and ischemic (HFimpEF: 17.2% vs. non-HFimpEF: 43.9%, p < 0.0001) etiologies. Multivariate analysis showed that non-ischemic etiologies significantly favored myocardial improvement compared to ischemic cardiomyopathy. NT-proBNP values were consistently higher in the non-HFimpEF group at all time points measured with statistically significant differences, except at admission. Event-free survival curves (hospitalization for HF, worsening HF, and all-cause mortality) diverged early, showing statistically significant differences between groups. Conclusions: Overall, 63% of patients hospitalized for de novo HFrEF achieved myocardial improvement within an average of 3-4 months, with improvement favored by valvular and tachycardiomyopathy etiologies. This improvement has a significant prognostic impact.
Keywords: NT-proBNP; de novo heart failure with reduced ejection fraction; improved ejection fraction; morbidity and mortality; predictors of recovery.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- McDonagh T.A., Metra M., Adamo M., Gardner R.S., Baumbach A., Böhm M., Burri H., Butler J., Čelutkienė J., Chioncel O., et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022;24:4–131. - PubMed
-
- Tsao C.W., Lyass A., Enserro D., Larson M.G., Ho J.E., Kizer J.R., Gottdiener J.S., Psaty B.M., Vasan R.S. Temporal Trends in the Incidence of and Mortality Associated with Heart Failure with Preserved and Reduced Ejection Fraction. JACC Heart Fail. 2018;6:678–685. doi: 10.1016/j.jchf.2018.03.006. - DOI - PMC - PubMed
-
- Heidenreich P.A., Bozkurt B., Aguilar D., Allen L.A., Byun J.J., Colvin M.M., Deswal A., Drazner M.H., Dunlay S.M., Evers L.R., et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e895–e1032. doi: 10.1161/CIR.0000000000001063. - DOI - PubMed
-
- Wilcox J.E., Fonarow G.C., Yancy C.W., Albert N.M., Curtis A.B., Heywood J.T., Inge P.J., McBride M.L., Mehra M.R., O’Connor C.M., et al. Factors associated with improvement in ejection fraction in clinical practice among patients with heart failure: Findings from IMPROVE HF. Am. Heart J. 2012;163:49–56.e2. doi: 10.1016/j.ahj.2011.10.001. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
