

Three Neglected STARD Criteria Reduce the Uncertainty of the Liver Fibrosis Biomarker FibroTest-T2D in Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD)
- PMID: 40428246
- PMCID: PMC12110081
- DOI: 10.3390/diagnostics15101253
Three Neglected STARD Criteria Reduce the Uncertainty of the Liver Fibrosis Biomarker FibroTest-T2D in Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD)
Abstract
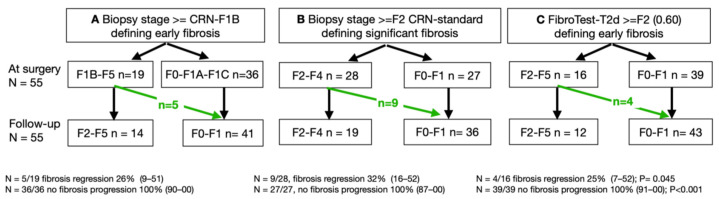
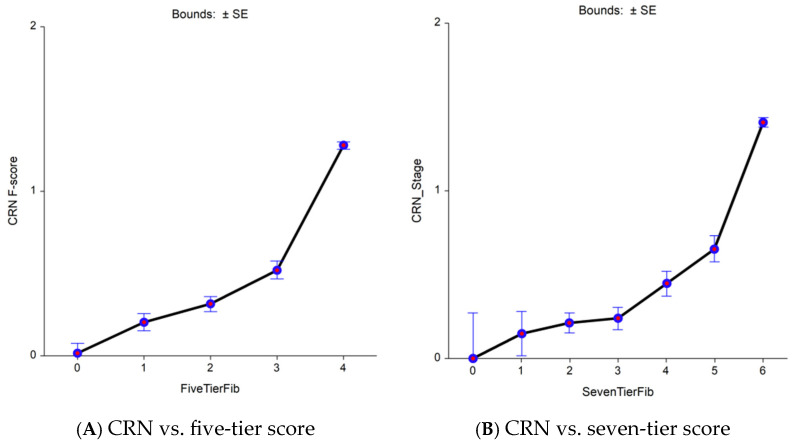
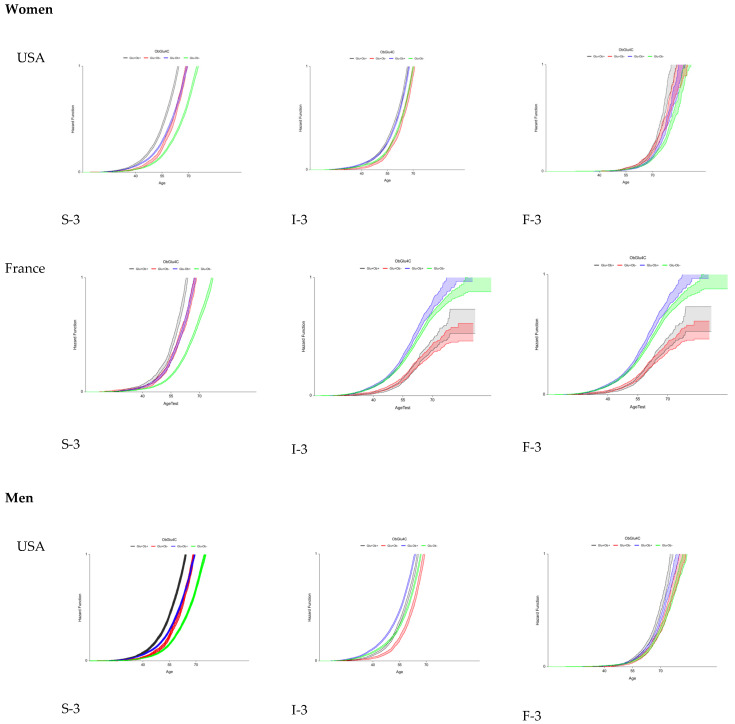
Background/Objectives: Bariatric surgery (BS), drugs approved for type-2-diabetes (T2D), obesity, and liver fibrosis (resmetirom) announce the widespread use of fibrosis tests in patients with metabolic liver disease (MASLD). An unmet need is to reduce the uncertainty of biomarkers for the diagnosis of the early stage of clinically significant fibrosis (eF). This can be achieved if three essential but neglected STARD methods (3M) are used, which have a more sensitive histological score than the standard comparator (five-tiers), the weighted area under the characteristic curve (wAUROC) instead of the binary AUROC, and biopsy length. We applied 3M to FibroTest-T2D to demonstrate this reduction of uncertainty and constructed proxies predicting eF in large populations. Methods: For uncertainty, seven subsets were analyzed, four included biopsies (n = 1903), and to assess eF incidence, three MASLD-populations (n = 299,098). FibroTest-T2D classification rates after BS and in outpatients-T2D (n = 402) were compared with and without 3M. In MASLD, trajectories of proxies and incidence against confounding factors used hazard ratios. Results: After BS (110 biopsies), reversal of eF was observed in 16/29 patients (84%) using seven-tier scores vs. 3/20 patients (47%) using five-tier scores (p = 0.005). When the biopsy length was above the median, FibroTest-T2D wAUROC was 0.90 (SD = 0.01), and the wAUROC was 0.88 (SD = 0.1) when the length was below the median (p < 0.001). For the first time, obesity was associated with eF before T2D (p < 0.001), and perimenopausal age with apoA1 and haptoglobin increases (p < 0.0001). Conclusions: Validations of circulating biomarkers need to assess their uncertainty. FibroTest-T2D predicts fibrosis regression after BS. Applying 3M and adjustments could avoid misinterpretations in MASLD surveillance.
Keywords: Obuchowski measure; UK BioBank; biopsy length; early liver fibrosis; granularity; uncertainty.
Conflict of interest statement
Thierry Poynard is the inventor of FibroTest and FibroTest-T2D and a fulltime employee and founder of BioPredictive, a spinoff of Sorbonne University that markets biomarkers. He is an emeritus professor at Sorbonne University. The tests’ patents belong to the public French organization “Assistance Publique Hôpitaux de Paris” and Sorbonne University. Olivier Deckmyn and Valentina Peta are full-time employees of BioPredictive. The other authors have no conflicts of interest. The RHU QUID-NASH project is funded by Agence Nationale de la Recherche Programme Investissements d’Avenir (grant ANR-17-T171105J-RHUS-0009 to D.V.). The RHU QUID NASH is implemented by Institut National de la Recherche Medicale, Paris Descartes University, Université Paris Cité, Centre National de la Recherche Scientifique, Centre de l’Energie Atomique, Servier, Biopredictive, and Assistance Publique-Hôpitaux de Paris.
Figures


Similar articles
-
Liver biopsy analysis has a low level of performance for diagnosis of intermediate stages of fibrosis.Clin Gastroenterol Hepatol. 2012 Jun;10(6):657-63.e7. doi: 10.1016/j.cgh.2012.01.023. Epub 2012 Feb 14. Clin Gastroenterol Hepatol. 2012. PMID: 22343514
-
Metabolic dysfunction-associated steatotic liver disease (MASLD) biomarkers and progression of lower limb arterial calcification in patients with type 2 diabetes: a prospective cohort study.Cardiovasc Diabetol. 2025 Apr 23;24(1):176. doi: 10.1186/s12933-025-02705-9. Cardiovasc Diabetol. 2025. PMID: 40269920 Free PMC article.
-
Prospective direct comparison of non-invasive liver tests in outpatients with type 2 diabetes using intention-to-diagnose analysis.Aliment Pharmacol Ther. 2023 Nov;58(9):888-902. doi: 10.1111/apt.17688. Epub 2023 Aug 29. Aliment Pharmacol Ther. 2023. PMID: 37642160
-
Accuracy of prognostic serological biomarkers in predicting liver fibrosis severity in people with metabolic dysfunction-associated steatotic liver disease: a meta-analysis of over 40,000 participants.Front Nutr. 2024 Feb 14;11:1284509. doi: 10.3389/fnut.2024.1284509. eCollection 2024. Front Nutr. 2024. PMID: 38419854 Free PMC article.
-
Epidemiology of metabolic dysfunction-associated steatotic liver disease.Clin Mol Hepatol. 2025 Feb;31(Suppl):S32-S50. doi: 10.3350/cmh.2024.0431. Epub 2024 Aug 19. Clin Mol Hepatol. 2025. PMID: 39159948 Free PMC article. Review.
References
-
- López Tórrez S.M., Ayala C.O., Ruggiro P.B., Costa C.A.D., Wagner M.B., Padoin A.V., Mattiello R. Accuracy of prognostic serological biomarkers in predicting liver fibrosis severity in people with metabolic dysfunction-associated steatotic liver disease: A meta-analysis of over 40,000 participants. Front. Nutr. 2024;11:1284509. doi: 10.3389/fnut.2024.1284509. - DOI - PMC - PubMed
-
- Syn N.L., Cummings D.E., Wang L.Z., Lin D.J., Zhao J.J., Loh M., Koh Z.J., Chew C.A., Loo Y.E., Tai B.C., et al. Association of metabolic–bariatric surgery with long-term survival in adults with and without diabetes: A one-stage meta-analysis of matched cohort and prospective controlled studies with 174 772 participants. Lancet. 2021;397:1830–1841. doi: 10.1016/S0140-6736(21)00591-2. - DOI - PubMed
-
- Lassailly G., Caiazzo R., Ntandja-Wandji L.-C., Gnemmi V., Baud G., Verkindt H., Ningarhari M., Louvet A., Leteurtre E., Raverdy V., et al. Bariatric Surgery Provides Long-term Resolution of Nonalcoholic Steatohepatitis and Regression of Fibrosis. Gastroenterology. 2020;159:1290–1301.e5. doi: 10.1053/j.gastro.2020.06.006. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
