

The Effect of a Kasai Procedure on Liver Transplantation in Children with Biliary Atresia: A Cohort Study
- PMID: 40429324
- PMCID: PMC12112731
- DOI: 10.3390/jcm14103328
The Effect of a Kasai Procedure on Liver Transplantation in Children with Biliary Atresia: A Cohort Study
Abstract
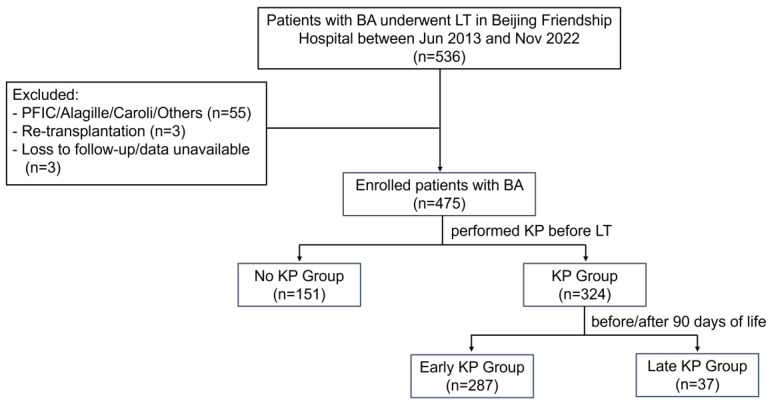
Background/Objectives: Biliary atresia (BA) is the most common etiology for pediatric liver transplantation (LT). However, whether a previous Kasai hepatoportoenterostomy (KP) and its timing influence the outcomes of BA patients who undergo LT remains controversial. Methods: Pediatric patients with BA who underwent LT at Beijing Friendship Hospital, Capital Medical University, between June 2013 and November 2022 were recruited. The patients were divided into non-KP, early-KP (before 90 days of life), and late-KP subgroups. The clinical data were compared among the groups. A nomogram to predict the 1-, 3-, and 5-year graft survival probabilities based on a multivariate Cox model was constructed and validated. Results: Among the 475 BA patients, the no-KP group accounted for 31.8%, the early KP for 60.4%, and the late KP for 7.8%, respectively. The incidences of LT complications were comparable among the groups. From the multivariate Cox analyses, an intensive care unit (ICU) stay and bleeding were identified as the independent risk factors for postoperative patient survival, and the LT type, graft type, vascular complications, and biliary complications were those for graft survival. A nomogram for graft survival was constructed, with a C-index of 0.82, and areas under the curves (AUCs) of 0.829, 0.824, and 0.824 for the 1-, 3-, and 5-year survival nomograms, respectively. The calibration and decision curve analysis (DCA) curves showed good discrimination ability and clinical applicability. A risk classification system was further developed, and the Kaplan-Meier curves demonstrated high discrimination between the high- and low-risk groups (p < 0.0001). Conclusions: A previous KP has no impact on patients or graft survival after LT in BA patients. The established nomogram may be helpful for counseling BA patients about their clinical prognosis after LT.
Keywords: Kasai hepatoportoenterostomy; biliary atresia; liver transplantation; nomogram; outcome.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Shi Y., Jiang Y.Z., Zhou G.P., Shi Y., Gan L.X., Kong Y.Y., Wang H.B., Zhu Z.J., Sun L.Y. Prognostic Factors Related to In-hospital Death in Children with Biliary Atresia: Analysis of a Nationwide Inpatient Database. J. Clin. Transl. Hepatol. 2023;11:416–424. doi: 10.14218/JCTH.2021.00456. - DOI - PMC - PubMed
-
- Tsuboi K., Watayo H., Tsukui T., Suda K., Abe E., Fujimoto T., Ochi T., Lane G.J., Koga H., Yamataka A. Native liver survivors of portoenterostomy for biliary atresia with excellent outcome: Redefining “successful” portoenterostomy. Pediatr. Surg. Int. 2022;39:24. doi: 10.1007/s00383-022-05313-w. - DOI - PubMed
-
- Kasahara M., Umeshita K., Sakamoto S., Fukuda A., Furukawa H., Sakisaka S., Kobayashi E., Tanaka E., Inomata Y., Kawasaki S., et al. Living donor liver transplantation for biliary atresia: An analysis of 2085 cases in the registry of the Japanese Liver Transplantation Society. Am. J. Transpl. 2018;18:659–668. doi: 10.1111/ajt.14489. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
