

Meta-Analytic Review of Coronary Angiography in Peri-Procedural Myocardial Injury and Infarction After Cardiac Surgery
- PMID: 40429400
- PMCID: PMC12111995
- DOI: 10.3390/jcm14103407
Meta-Analytic Review of Coronary Angiography in Peri-Procedural Myocardial Injury and Infarction After Cardiac Surgery
Abstract
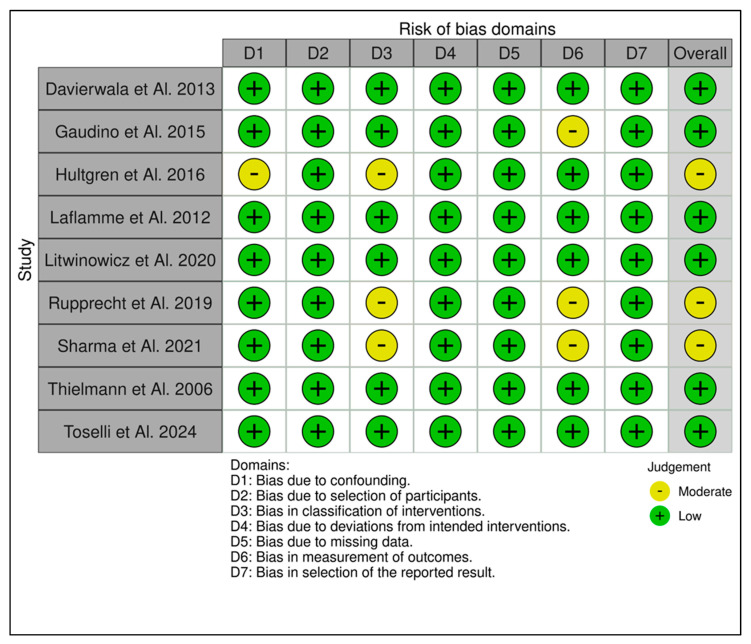
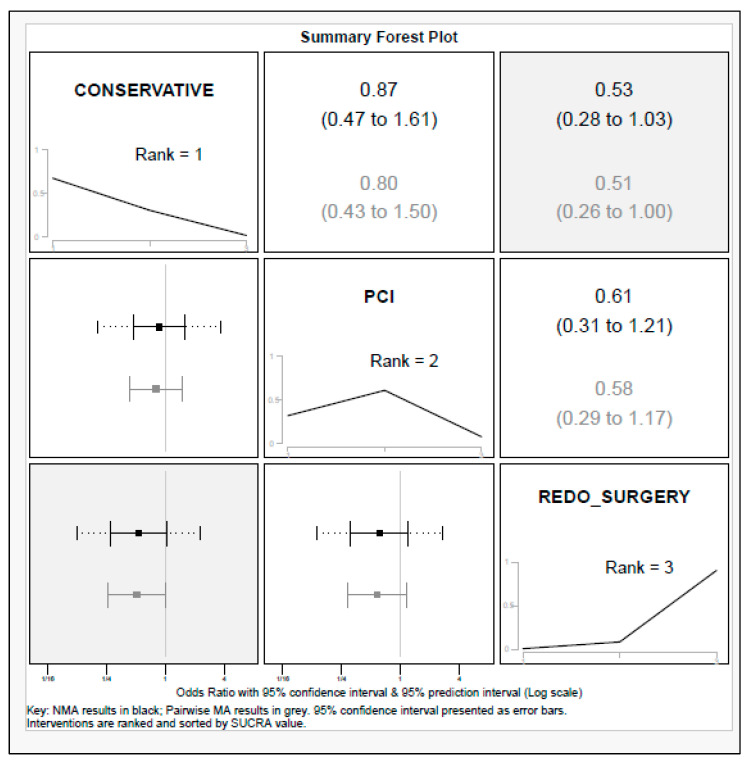
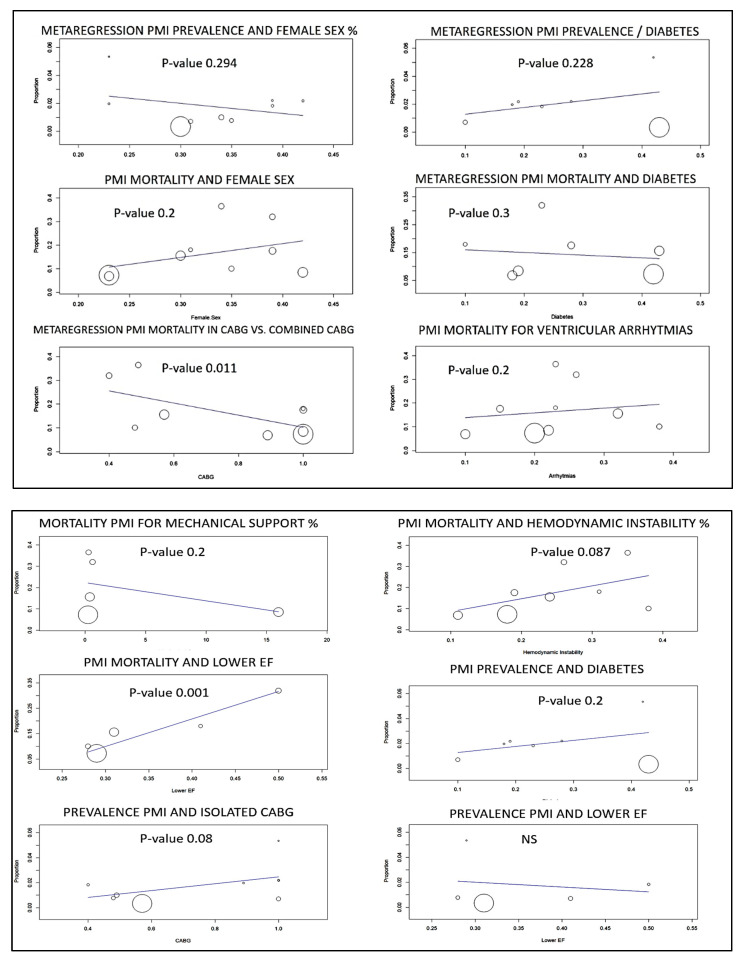
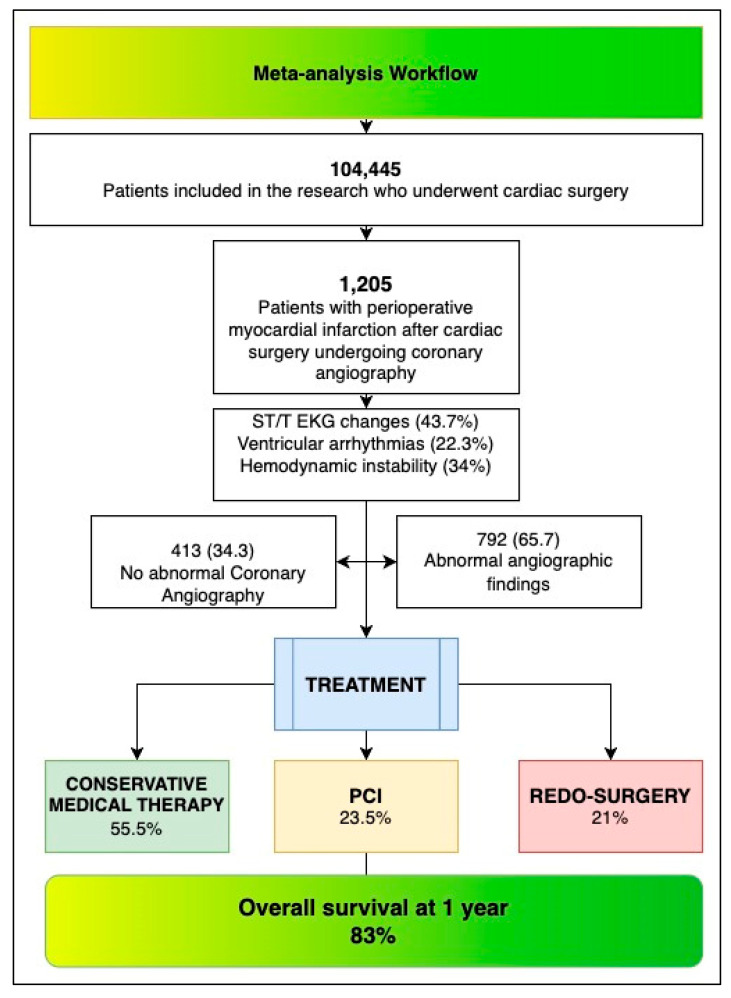
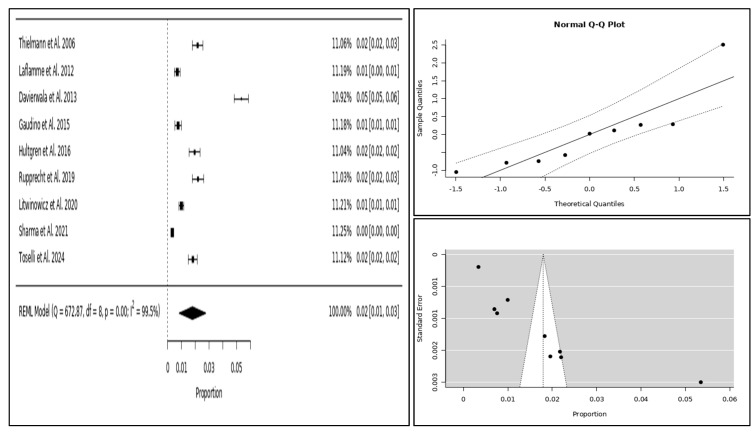
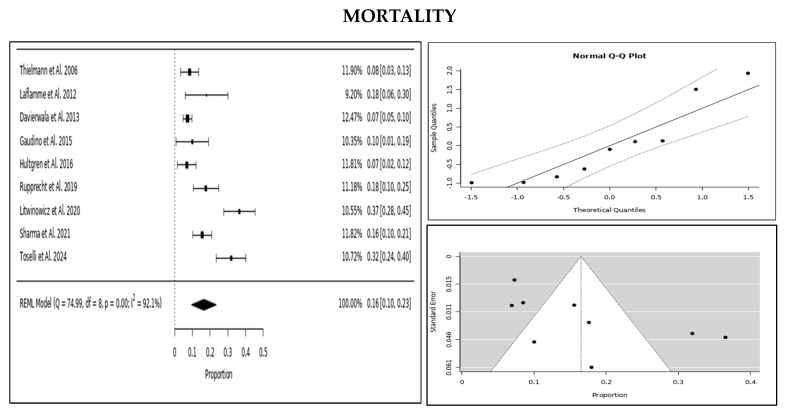
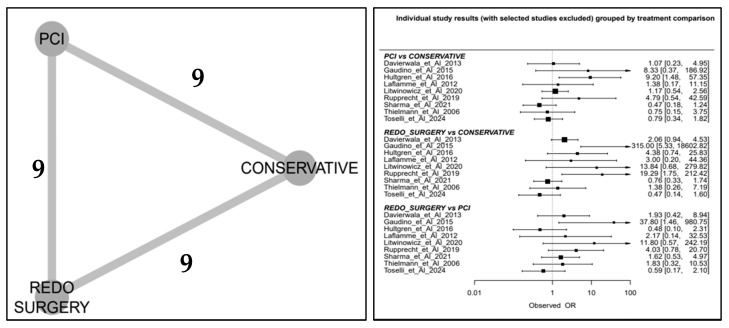
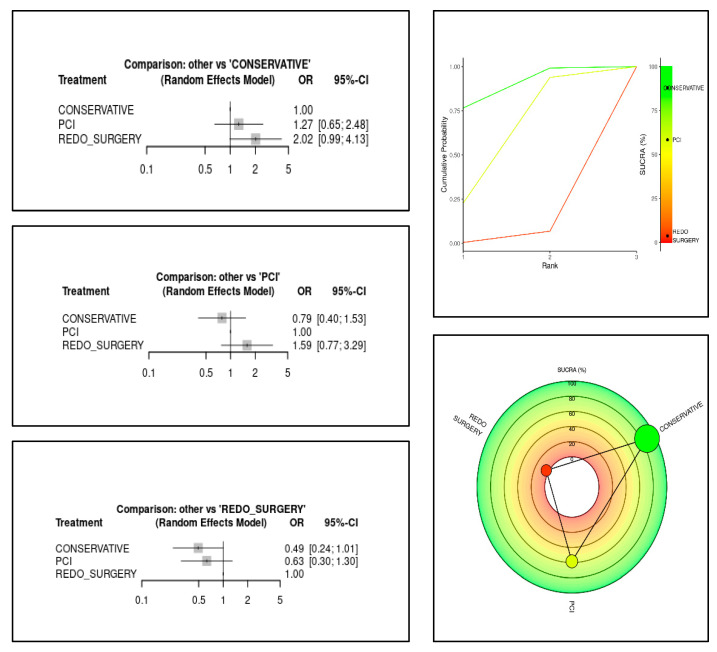
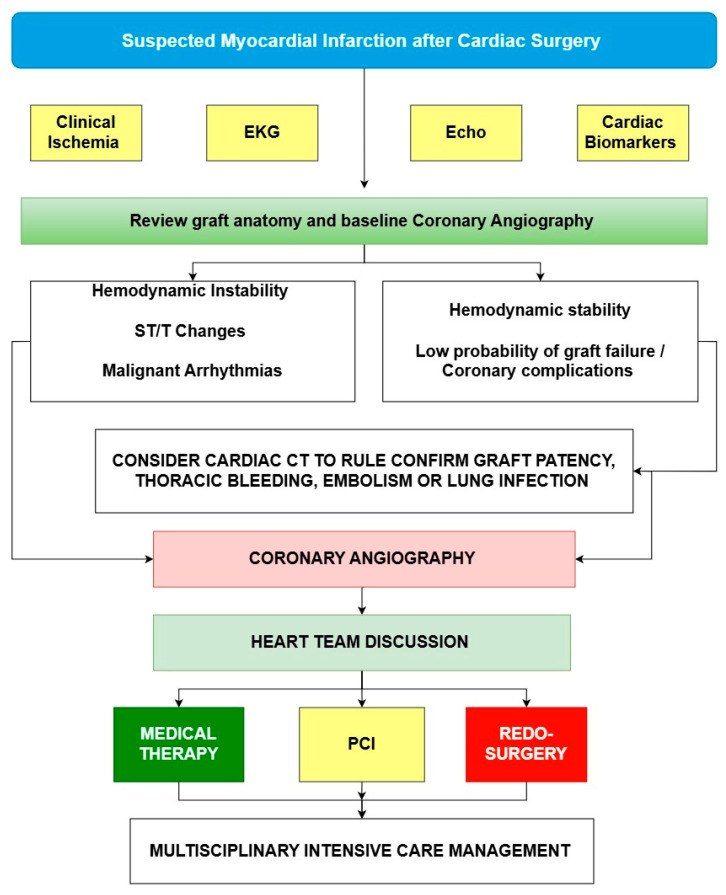
Introduction: Peri-procedural myocardial infarction (PMI) after cardiac surgery is a significant yet often under-recognised complication, sometimes necessitating urgent coronary angiography (PMI-rCA). This meta-analysis evaluates its prevalence, angiographic findings, management strategies, and associated mortality. Methods: A systematic review and meta-analysis were conducted according to PRISMA guidelines. Data from nine studies comprising 104,445 post-cardiac surgery patients were analysed. Among them, those undergoing PMI-rCA were categorised by treatment strategy: conservative management, percutaneous coronary intervention (PCI), or reperform surgery. A network meta-analysis compared mortality risks across these groups, with findings visualised using forest plots, network diagrams, and SUCRA rankings. Results: PMI-rCA was performed in 1205 patients (2%). Of these, 34.3% had no significant angiographic abnormalities, 53.7% exhibited graft failure, and 10.4% had native vessel ischemia. Management strategies included conservative treatment (55.5%), PCI (23.5%), and reperforming surgery (21%). Network meta-analysis indicated that conservative management was associated with the lowest mortality risk, followed by PCI, while reperforming surgery had the highest risk. Discussion: These findings highlight the complexity of PMI diagnosis and treatment. The high proportion of patients without significant angiographic abnormalities raises concerns about potential overuse of invasive procedures. Meanwhile, PCI appears to be a more favourable interventional strategy than reperforming surgery in terms of mortality outcomes. Conclusions: PMI requiring coronary angiography is uncommon but clinically significant, with a 16% mortality rate. A tailored, risk-based approach is essential to optimise management, balancing conservative therapy, PCI, and reperforming surgery based on individual patient profiles.
Keywords: cardiac surgery complications; graft failure; percutaneous coronary intervention (PCI); peri-procedural myocardial infarction requiring coronary angiography; surgical mortality and outcomes.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Impact of Peri-Procedural Myocardial Infarction on Outcomes After Revascularization.J Am Coll Cardiol. 2020 Oct 6;76(14):1622-1639. doi: 10.1016/j.jacc.2020.08.009. J Am Coll Cardiol. 2020. PMID: 33004127 Clinical Trial.
-
Intravascular ultrasound to guide percutaneous coronary interventions: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(12):1-97. Epub 2006 Apr 1. Ont Health Technol Assess Ser. 2006. PMID: 23074482 Free PMC article.
-
Percutaneous Intervention for Myocardial Infarction After Noncardiac Surgery: Patient Characteristics and Outcomes.J Am Coll Cardiol. 2016 Jul 26;68(4):329-38. doi: 10.1016/j.jacc.2016.03.602. J Am Coll Cardiol. 2016. PMID: 27443427
-
Control angiography for perioperative myocardial Ischemia after coronary surgery: meta-analysis.J Cardiothorac Surg. 2018 Feb 27;13(1):24. doi: 10.1186/s13019-018-0710-0. J Cardiothorac Surg. 2018. PMID: 29482583 Free PMC article. Review.
-
The clinical approach to diagnosing peri-procedural myocardial infarction after percutaneous coronary interventions according to the fourth universal definition of myocardial infarction - from the study group on biomarkers of the European Society of Cardiology (ESC) Association for Acute CardioVascular Care (ACVC).Biomarkers. 2022 Jul;27(5):407-417. doi: 10.1080/1354750X.2022.2055792. Epub 2022 May 26. Biomarkers. 2022. PMID: 35603440 Free PMC article. Review.
References
-
- Gaudino M., Dangas G.D., Angiolillo D.J., Brodt J., Chikwe J., DeAnda A., Hameed I., Rodgers M.L., Sandner S., Sun L.Y., et al. Considerations on the Management of Acute Postoperative Ischemia After Cardiac Surgery: A Scientific Statement from the American Heart Association. Circulation. 2023;148:442–454. doi: 10.1161/CIR.0000000000001154. - DOI - PubMed
-
- Gaudino M., Flather M., Capodanno D., Milojevic M., Bhatt D.L., Biondi Zoccai G., Boden W.E., Devereaux P.J., Doenst T., Farkouh M., et al. European Association of Cardio-Thoracic Surgery (EACTS) expert consensus statement on perioperative myocardial infarction after cardiac surgery. Eur. J. Cardiothorac. Surg. 2024;65:ezad415. doi: 10.1093/ejcts/ezad415. - DOI - PubMed
-
- Nanni S., Garofalo M., Schinzari M., Nardi E., Semprini F., Battistini P., Barberini F., Foà A., Baiocchi M., Castelli A., et al. Prognostic value of high-sensitivity cardiac troponin I early after coronary artery bypass graft surgery. J. Cardiothorac. Surg. 2022;17:280. doi: 10.1186/s13019-022-02027-x. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
