

Real-World Implementation of PRISMA-7 and Clinical Frailty Scale for Frailty Identification and Integrated Care Activation: A Cross-Sectional Study in Northern Italian Primary Practice
- PMID: 40429424
- PMCID: PMC12111854
- DOI: 10.3390/jcm14103431
Real-World Implementation of PRISMA-7 and Clinical Frailty Scale for Frailty Identification and Integrated Care Activation: A Cross-Sectional Study in Northern Italian Primary Practice
Abstract
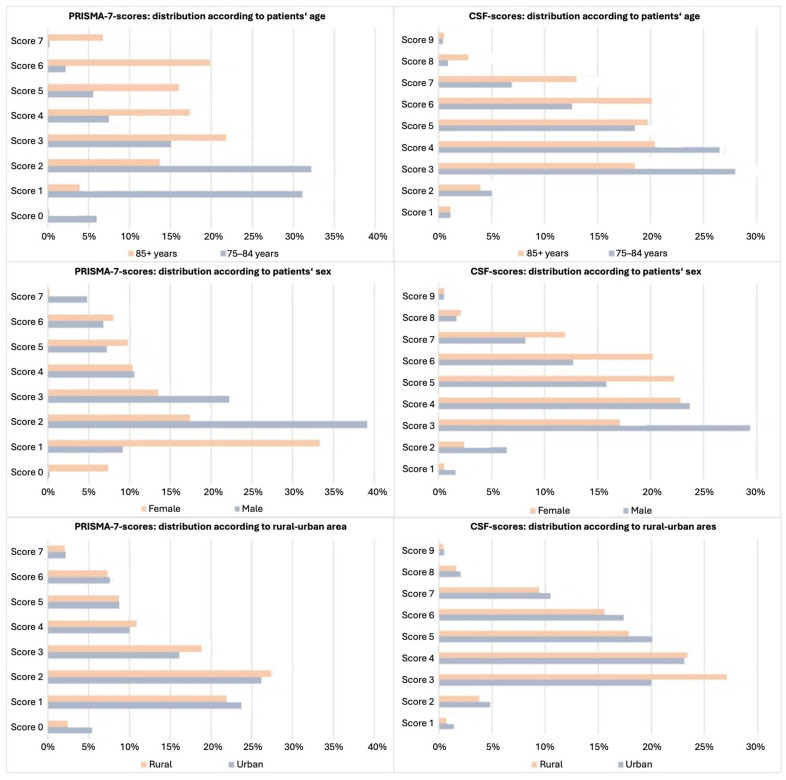
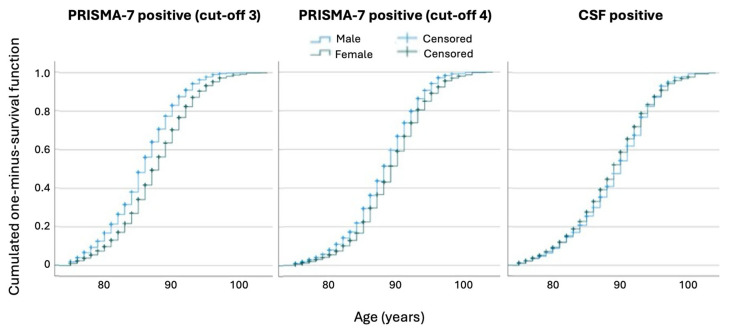
Background/Objectives: Frailty screening is crucial for identifying vulnerable older adults who may benefit from interventions. However, the implementation of screening in primary care and integration into personalised care pathways remains limited. This study examined the feasibility of a two-step frailty screening approach combining PRISMA-7 and the Clinical Frailty Scale (CFS). The study assessed PRISMA-7 cut-offs' impact on frailty classification, CFS agreement, and activation of integrated domiciliary care. Methods: This cross-sectional study was conducted in Northern Italy. General practitioners screened patients aged ≥75 years using the PRISMA-7 tool; if the result was positive (score ≥ 3), the Clinical Frailty Scale (CFS) was subsequently applied. Descriptive statistics, group comparisons, correlation analyses, and logistic regression models were employed to evaluate the predictors of frailty and activation of integrated domiciliary care. Comparisons were made for PRISMA-7 cut-off values ≥3 and ≥4. Results: Among the 18,658 patients evaluated using PRISMA-7, 46.0% were identified as frail with a threshold of ≥3 and 28.8% with ≥4. In a subset of 7970 patients assessed using both PRISMA-7 and the Clinical Frailty Scale (CFS), CFS confirmed frailty (score ≥ 5) in 48.3% of the patients at a PRISMA-7 cut-off of three and 68.2% at a cut-off of four. The female sex predicted frailty by CFS, whereas the male sex was correlated with frailty at the PRISMA-7 cut-off of three. Rural location was correlated with frailty by PRISMA-7 but showed an inverse relationship with frailty by CFS. Integrated domiciliary care began in 14.2% of the patients meeting the clinical criteria, with a higher frequency in rural areas. Concordance between PRISMA-7 and CFS increased with patient age, and at a cut-off of four. Conclusions: Two-step frailty screening using PRISMA-7 and CFS is viable for primary care. Using a PRISMA-7 cut-off score of ≥4 may reduce frailty overestimation, enhance congruence with clinical assessments, and reduce sex-related bias. These findings support incorporating structured screening into personalised care planning and refining frailty tools to improve equity and effectiveness.
Keywords: Clinical Frailty Scale; PRISMA-7; frailty screening; integrated domiciliary care; personalised medicine; primary care.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the study design; collection, analyses, or interpretation of data; writing of the manuscript; or decision to publish the results.
Figures
References
-
- Hoogendijk E.O., van der Horst H.E., Deeg D.J.H., Frijters D.H.M., Prins B.A.H., Jansen A.P.D., Nijpels G., van Hout H.P.J. The Identification of Frail Older Adults in Primary Care: Comparing the Accuracy of Five Simple Instruments. Age Ageing. 2013;42:262–265. doi: 10.1093/ageing/afs163. - DOI - PubMed
-
- Boucher E.L., Gan J.M., Rothwell P.M., Shepperd S., Pendlebury S.T. Prevalence and Outcomes of Frailty in Unplanned Hospital Admissions: A Systematic Review and Meta-Analysis of Hospital-Wide and General (Internal) Medicine Cohorts. eClinicalMedicine. 2023;59:101947. doi: 10.1016/j.eclinm.2023.101947. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
