

Risk Factors in Patients Who Had Prior Renal or Liver Transplant Undergoing Primary Total Hip Arthroplasty
- PMID: 40429481
- PMCID: PMC12111864
- DOI: 10.3390/jcm14103486
Risk Factors in Patients Who Had Prior Renal or Liver Transplant Undergoing Primary Total Hip Arthroplasty
Abstract
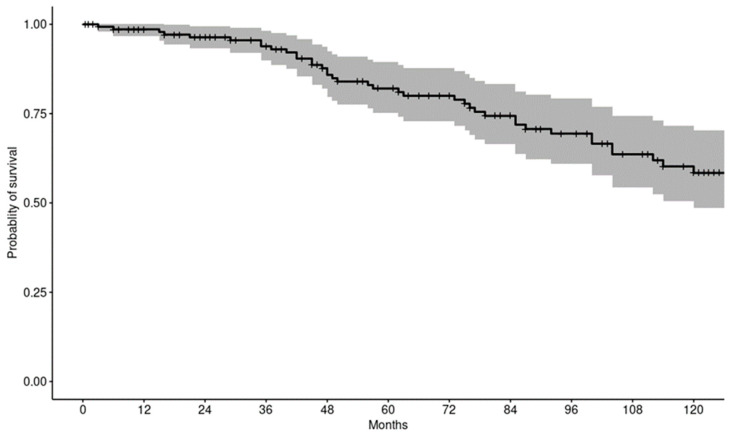
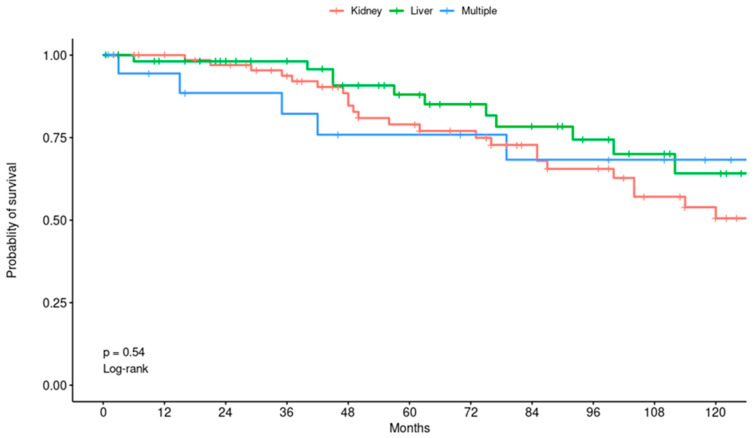
Background: Solid organ transplant (SOT) recipients are living longer and, consequently, more of them require elective total hip arthroplasty (THA) to restore mobility and improve quality of life. Because these patients are chronically immunosuppressed and often burdened by multiple comorbidities, their peri-operative risk profile may differ substantially from that of the general THA population. This study aimed to evaluate risk factors associated with acute medical and surgical complications, implant survivorship, and overall mortality in patients with a history of SOT who underwent THA. Methods: A total of 173 THA procedures were reviewed in patients with previous SOT. Among them, 64 had undergone liver transplantation (LT), 83 had received renal transplants (RT), and 26 had experienced more than one type of organ transplant (MT). Kaplan-Meier survival analysis was employed to estimate median survival. Complications were examined using univariate analysis through mixed-effects logistic regression, while Cox regression was utilized to assess mortality risk. The median follow-up period extended to 99 months. Results: The proportion of patients experiencing at least one acute medical event was 27% in the LT group, 33% in the RT group, and 38% in the MT group, with no statistically significant difference between groups (p = 0.5). American Society of Anesthesiologists Class (ASA) 4 (Odds Ratio (OR) = 28; p = 0.006) and treatment with bisphosphonates (OR = 2.25; p = 0.03) were associated with higher risk of acute medical complications. Increased age at the time of SOT was linked to a reduced likelihood of surgical complications (OR = 0.94, p = 0.008), as was older age at the time of undergoing THA (OR = 0.92, p = 0.001). The observed rates of reoperation and implant revision were 3% and 1%, respectively. The estimated patient survivorship rates at 1, 5, and 10 years were 98.6, 82, and 58.4%, respectively. Older age at SOT (Hazard Ratio (HR) = 1.06, p < 0.001), at THA (HR = 1.08, p < 0.001), ASA 4 at THA (HR = 7.57, p = 0.02), and atrial fibrillation (AFib) (HR = 3.13, p = 0.02) were associated with higher mortality. Conclusions: ASA 4 and bisphosphonates were associated with a higher risk of acute medical complications, whereas older age was associated with lower surgical complications. Additionally, older age, ASA 4, and AFib were associated with higher mortality.
Keywords: kidney transplantation; liver transplantation; postoperative complications; survival analysis; total hip arthroplasty.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- United Network for Organ Sharing (UNOS) Website Organ Transplantation Community and UNOS Member Community. [(accessed on 1 January 2025)]. Available online: https://unos.org/news/2022-organ-transplants-again-set-annual-records/
-
- Scientific Registry of Transplant Recipients (SRTR) Website The OPTN/SRTR Annual Data Report. [(accessed on 1 January 2025)];2021 Available online: https://srtr.transplant.hrsa.gov/adr/adr2021.
-
- Navale S.M., Szubski C.R., Klika A.K., Schiltz N.K., Desai P.P., Barsoum W.K. The impact of solid organ transplant history on inpatient complications, mortality, length of stay, and cost for primary total hip arthroplasty admissions in the United States. J. Arthroplast. 2017;32:1107–1116. doi: 10.1016/j.arth.2016.10.017. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
