

Personalized Nutrition Strategies for Patients in the Intensive Care Unit: A Narrative Review on the Future of Critical Care Nutrition
- PMID: 40431399
- PMCID: PMC12114248
- DOI: 10.3390/nu17101659
Personalized Nutrition Strategies for Patients in the Intensive Care Unit: A Narrative Review on the Future of Critical Care Nutrition
Abstract
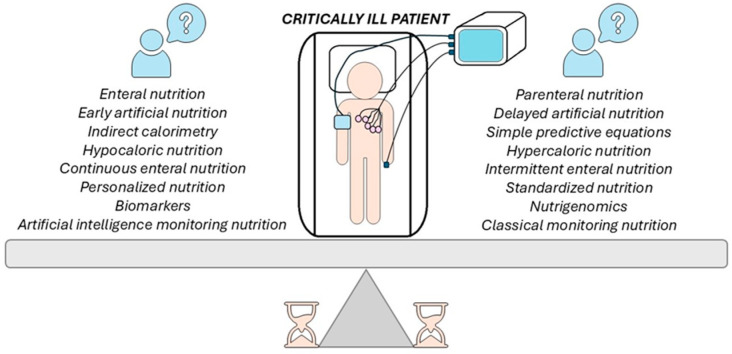
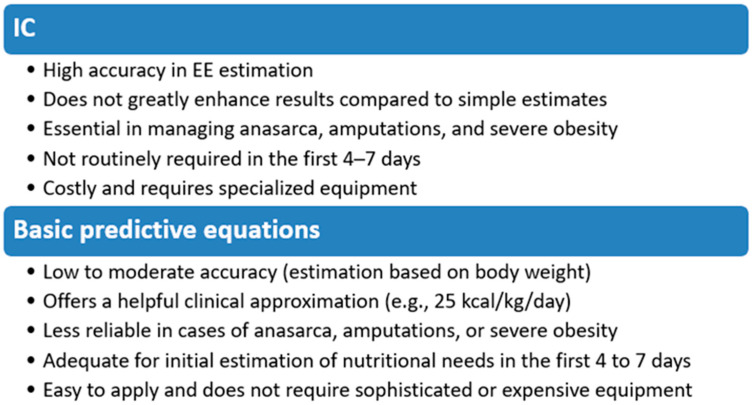
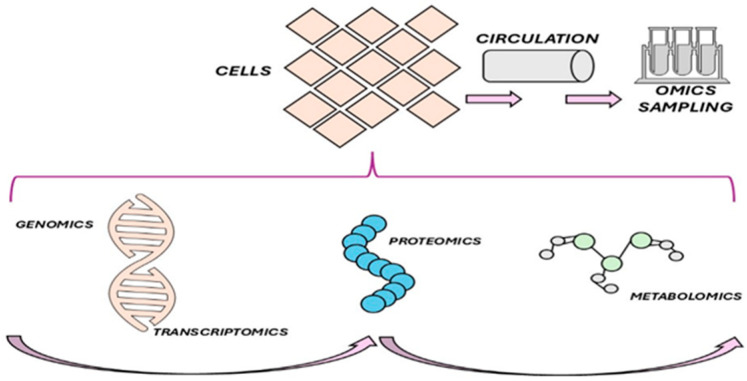
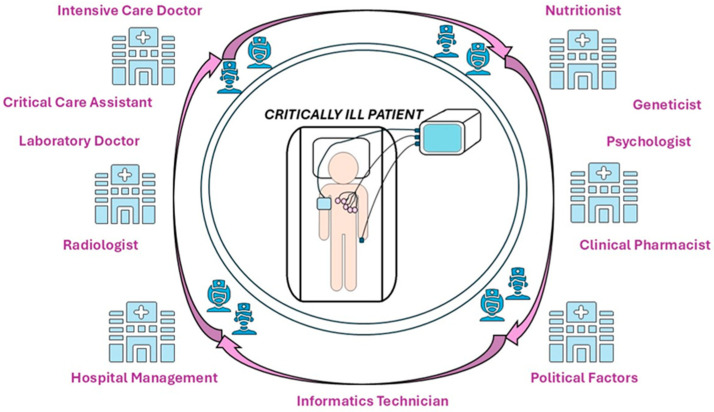
Introduction: Critically ill patients in intensive care units (ICUs) are at high risk of malnutrition, which can result in muscle atrophy, polyneuropathy, increased mortality, or prolonged hospitalizations with complications and higher costs during the recovery period. They often develop ICU-acquired weakness, exacerbated by sepsis, immobilization, and drug treatments, leading to rapid muscle mass loss and long-term complications. Studies indicate that adequate protein and calorie intake can decrease mortality and improve prognosis and recovery. However, optimal implementation remains a critical challenge. Objectives: This narrative review aims to summarize recent advances in nutritional strategies for critically ill patients. It highlights the benefits and limitations of current approaches including enteral (EN) and parenteral nutrition (PN) and examines their impact on clinical outcomes and overall mortality. Additionally, the review explores the emerging role of precision nutrition in critical care using technologies such as metabolomics and artificial intelligence (AI) to provide valuable insights into optimizing nutritional care in critically ill patients. Methods: A comprehensive literature search was conducted to identify recent studies, clinical guidelines, and expert consensus papers on nutritional support for ICU patients. The investigation focused on critical aspects such as the optimal timing for intervention, the route of administration, specific protein and energy targets, and technological innovations to support personalized nutrition, ensuring that each patient receives tailored support based on their unique needs. Results: Guidelines recommend initiating EN or PN nutrition within the first 48 h of admission, using indirect calorimetry (IC) to estimate energy needs, and supplementing protein up to 1.2 g/kg/day after stabilization. IC has gained importance in assessing energy needs but is still underused in the ICU. EN is preferred because it maintains intestinal integrity, reduces the risk of infections, and is recommended within the first 48 h of ICU admission. PN is used when EN is infeasible, but it increases the risk of infection. By integrating metabolomics with transcriptomic and genomic data, we can gain a deeper understanding of the effect of nutrition on cellular homeostasis, facilitating personalized treatments and enhancing the recovery of critically ill patients. Conclusions: AI is becoming increasingly important in monitoring and evaluating artificial nutrition, providing a more accurate and efficient alternative to traditional methods. AI can assist in identifying and managing malnutrition and is effective for estimating caloric and nutrient intake. AI minimizes human error, enables continuous monitoring, and integrates various data sources. The nutritional care of critically ill patients requires collaboration among specialists from diverse fields, including physicians, nutritionists, pharmacists, radiologists, IT experts, and policymakers.
Keywords: critical illness; enteral and parenteral nutrition; metabolic diseases; metabolome; nutritional genomics; personalized nutrition.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Cass A.R., Charlton K.E. Prevalence of Hospital-Acquired Malnutrition and Modifiable Determinants of Nutritional Deterioration during Inpatient Admissions: A Systematic Review of the Evidence. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2022;35:1043–1058. doi: 10.1111/jhn.13009. - DOI - PMC - PubMed
-
- White J.V., Guenter P., Jensen G., Malone A., Schofield M., Academy Malnutrition Work Group ASPEN Malnutrition Task Force; A.S.P.E.N. Board of Directors. Consensus Statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: Characteristics Recommended for the Identification and Documentation of Adult Malnutrition (Undernutrition) JPEN J. Parenter. Enter. Nutr. 2012;36:275–283. doi: 10.1177/0148607112440285. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
