

Diagnostic Performance of Clinical Metagenomic Next-Generation Sequencing for Suspected Central Nervous System Infections in a Municipal Hospital: A Retrospective Study in China
- PMID: 40432811
- PMCID: PMC12106916
- DOI: 10.2147/IDR.S500279
Diagnostic Performance of Clinical Metagenomic Next-Generation Sequencing for Suspected Central Nervous System Infections in a Municipal Hospital: A Retrospective Study in China
Abstract
Purpose: Cerebrospinal fluid (CSF) metagenomic next-generation sequencing (mNGS) has the potential to identify the majority of pathogens in a single test. Accurate pathogen identification is vital for central nervous system infection (CNSi). However, there are few related studies investigating in a municipal hospital.
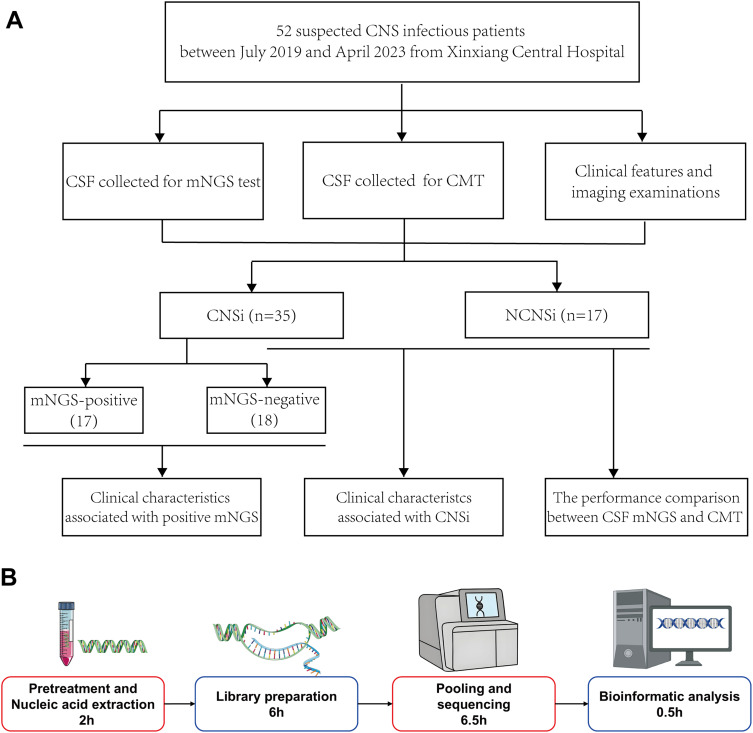
Patients and methods: A total of 52 suspected CNSi patients were retrospectively recruited in Xinxiang central hospital between July 2019 and April 2023. The diagnostic performance of CSF mNGS, conventional microbiological tests (CMT), and the combination of CSF mNGS and CMT were evaluated by comparing to the final diagnosis.
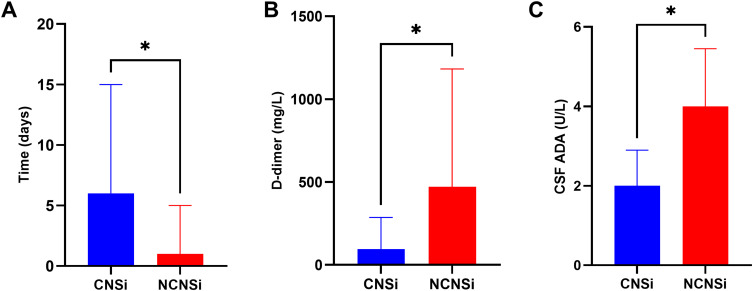
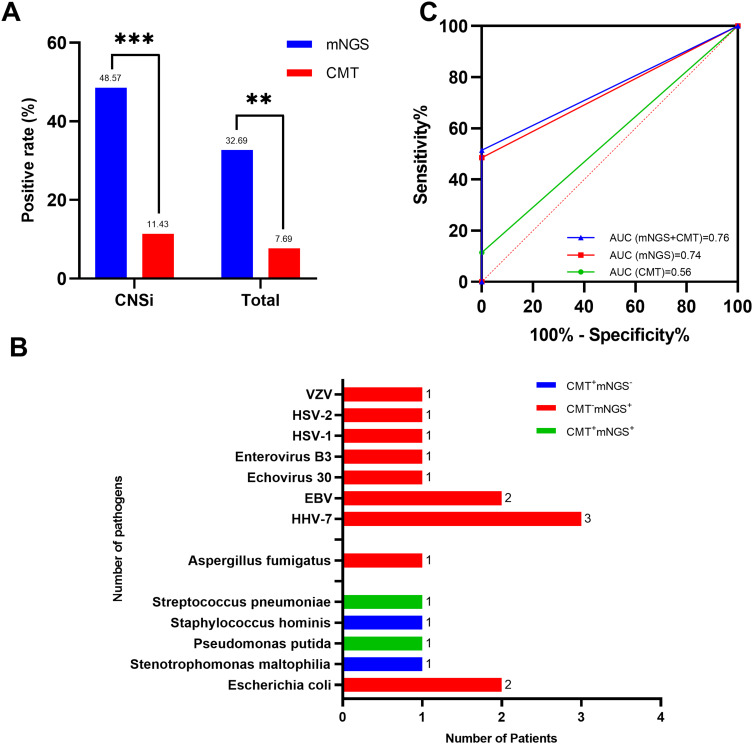
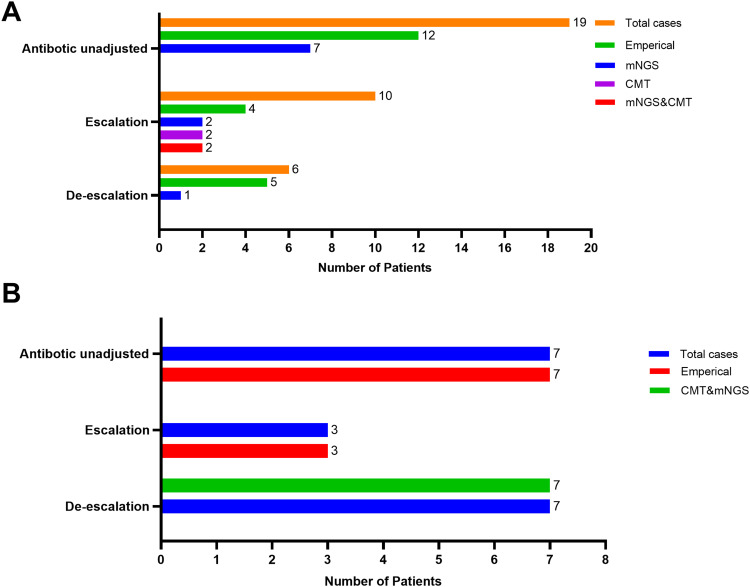
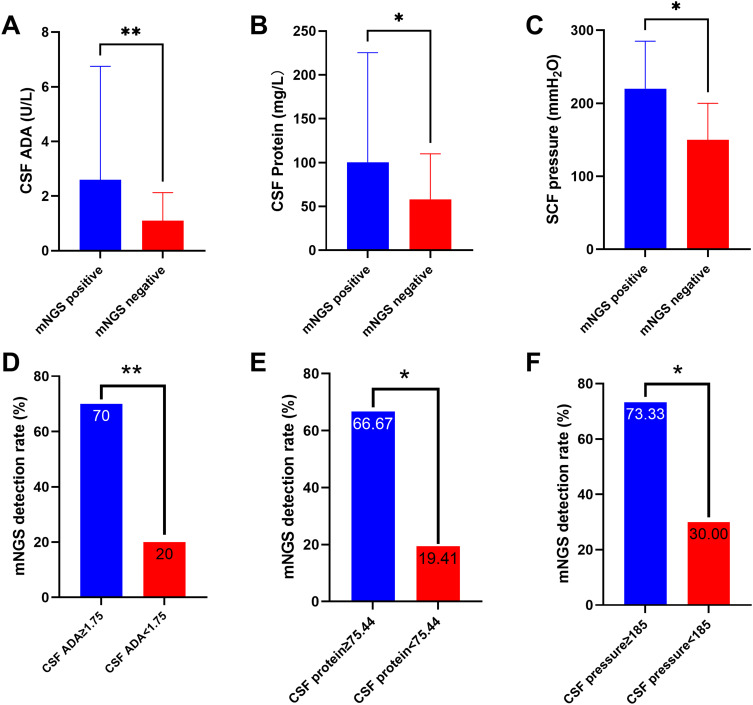
Results: Among 52 suspected CNSi patients, 35 were diagnosed as CNSi. In comparison to the final diagnosis, the area under curves (AUC) for CSF CMT, CSF mNGS, and the combination of CMT and mNGS for the diagnosis of CNSi were 0.56 (95% CI 0.4-0.72), 0.74 (95% CI 0.61-0.84), and 0.76 (95% CI 0.63-0.88), respectively. The sensitivities were 11.43% (95% CI 4.54%-25.95%), 48.57% (95% CI 32.99%-64.43%), and 51.43% (95% CI 35.57%-67.01%), respectively. The accuracy was 40.38 (95% CI 27.01%-54.90%), 65.38% (95% CI 50.91%-78.03%), and 67.31% (95% CI 52.89%-79.67%), respectively. Furthermore, based on CSF mNGS results, seven patients confirmed initial treatment, two escalated, and one de-escalated. Additionally, we identified the optimal cutoff values as 1.75 U/L for CSF adenosine deaminase (ADA), 75.44 U/L for CSF protein, and 185 mmH2O for CSF pressure, when these values were exceeded, CSF mNGS tended to yield positive results.
Conclusion: CSF mNGS showed superior diagnostic performance in CNSi and hence could serve as a complementary tool to CMT and conjunctively guide the precision therapy. Additionally, the values for CSF ADA, protein and pressure could assist in predicting mNGS positive result. With technical improvements for mNGS sample processing to increase throughput and reduce costs, clinicians may use mNGS more widely in municipal hospital laboratories.
Keywords: CMT; CNS infections; CSF; conventional microbiological tests; mNGS.
© 2025 Wang et al.
Conflict of interest statement
The author(s) report no conflicts of interest in this work.
Figures
Similar articles
-
The clinical utility of metagenomic next-generation sequencing for the diagnosis of central nervous system infectious diseases.Neurol Res. 2023 Oct;45(10):919-925. doi: 10.1080/01616412.2023.2247299. Epub 2023 Aug 24. Neurol Res. 2023. PMID: 37615407
-
An Investigation into Diagnostic Strategies for Central Nervous System Infections Through the Integration of Metagenomic Next-Generation Sequencing and Conventional Diagnostic Methods.Infect Drug Resist. 2024 Nov 5;17:4865-4873. doi: 10.2147/IDR.S483985. eCollection 2024. Infect Drug Resist. 2024. PMID: 39524979 Free PMC article.
-
A single-center, retrospective study of hospitalized patients with lower respiratory tract infections: clinical assessment of metagenomic next-generation sequencing and identification of risk factors in patients.Respir Res. 2024 Jun 20;25(1):250. doi: 10.1186/s12931-024-02887-y. Respir Res. 2024. PMID: 38902783 Free PMC article.
-
Diagnostic performance of metagenomic next-generation sequencing for the detection of pathogens in cerebrospinal fluid in pediatric patients with central nervous system infection: a systematic review and meta-analysis.BMC Infect Dis. 2024 Jan 18;24(1):103. doi: 10.1186/s12879-024-09010-y. BMC Infect Dis. 2024. PMID: 38238719 Free PMC article.
-
Clinical Metagenomic Next-Generation Sequencing for Diagnosis of Central Nervous System Infections: Advances and Challenges.Mol Diagn Ther. 2024 Sep;28(5):513-523. doi: 10.1007/s40291-024-00727-9. Epub 2024 Jul 11. Mol Diagn Ther. 2024. PMID: 38992308 Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
