

Efficacy of a Graftless Salter Osteotomy in Developmental Dysplasia of the Hip
- PMID: 40432865
- PMCID: PMC12088171
- DOI: 10.1016/j.jposna.2025.100188
Efficacy of a Graftless Salter Osteotomy in Developmental Dysplasia of the Hip
Abstract
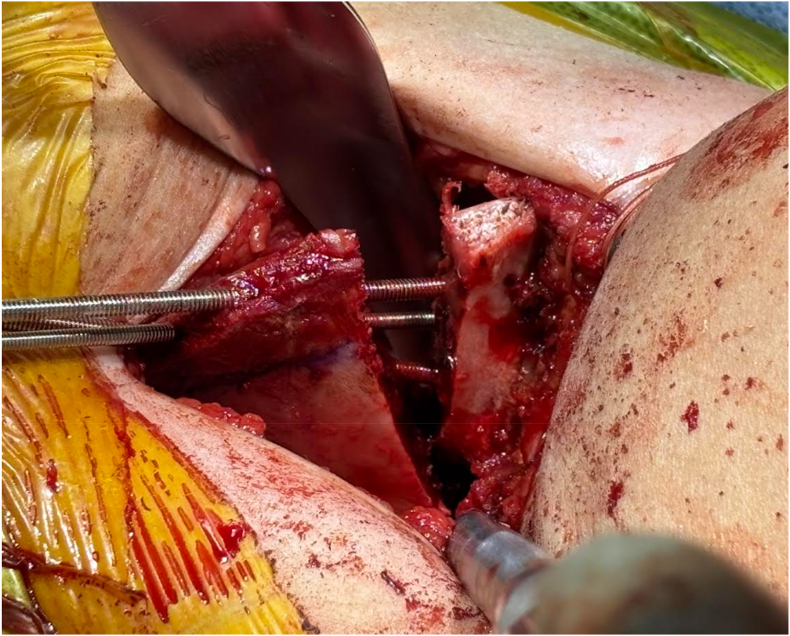
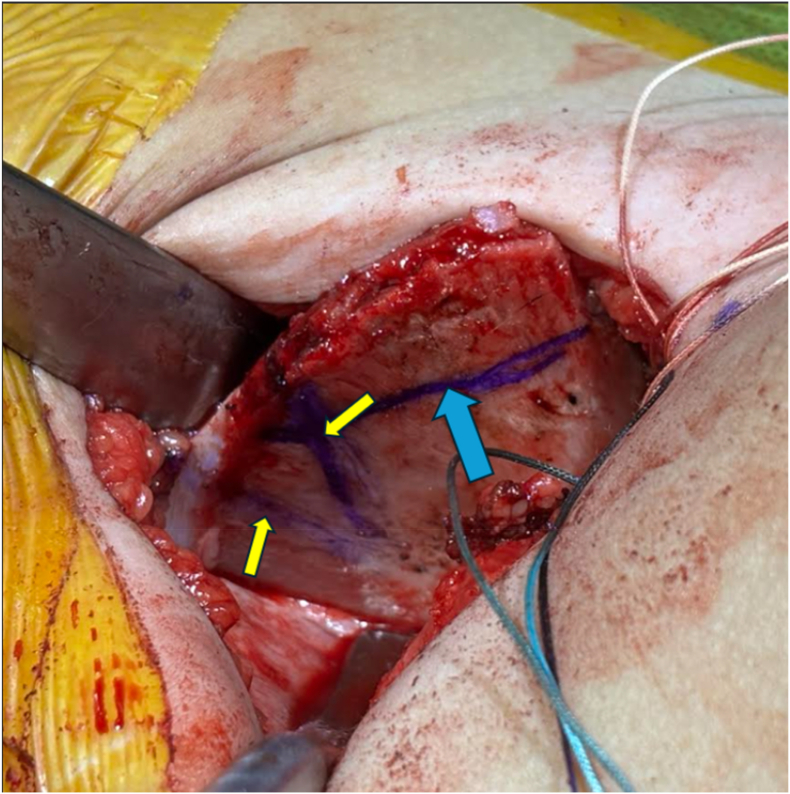
Background: Salter's innominate osteotomy is one of the most popular pediatric hip procedures for developmental dysplasia of the hip (DDH). Traditionally, Salter osteotomies require harvesting of autograft from the iliac crest, which can result in iliac wing deformities, pelvic asymmetry, and abductor dysfunction. A graftless variation of this procedure has been described in which the iliac osteotomy is fixed with threaded pins without an intervening graft, but literature surrounding this technique is sparse. The purpose of this study was to evaluate the efficacy of a graftless Salter osteotomy and compare the degree of correction to the traditional method.
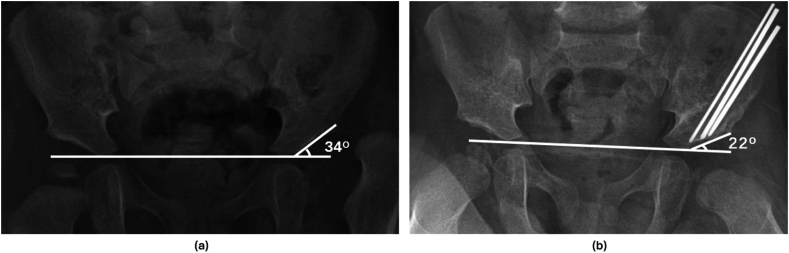
Methods: A retrospective review was performed of all Salter osteotomies performed at a single tertiary care children's hospital from 2009 to 2024. Demographic and clinical variables were extracted from electronic medical records. Acetabular indices (AIs) on preoperative and 3-month postoperative AP pelvic radiographs were compared to assess the degree of acetabular correction. Traditional and graftless procedures were propensity score matched 1:2 based on age, gender, and preoperative AI. Acetabular correction was compared between the two cohorts using the Wilcoxon Mann-Whitney test.
Results: Forty-seven hips were identified (14 traditional, 33 graftless). Seventy-two percent of patients were female; the mean age at surgery was 29.9 months (range: 15-70). Thirty-eight hips (81%) underwent concomitant open reduction. Propensity score matched analysis demonstrated no significant difference in the degree of acetabular correction between the cohorts (traditional vs graftless: 11.9° ± 5.4 vs 12.7° ± 5.7, P = .69). All osteotomies healed by 3 months, and there were no cases of lost fixation with either technique.
Conclusions: The graftless variation of Salter's osteotomy yields a comparable degree of acetabular correction to the traditional technique. There were no complications in either cohort from the osteotomy. The graftless Salter osteotomy is a safe and effective alternative to the traditional Salter osteotomy without the risk of iliac wing deformities and potential abductor dysfunction.
Key concepts: (1)Graftless Salter osteotomy provides similar degrees of correction to the traditional technique.(2)No complications related to the osteotomy were observed in both the graftless and traditional cohort.(3)All Salter osteotomies demonstrated healing at the 3-month postoperative timepoint.
Level of evidence: IV.
Keywords: DDH; Pelvic osteotomy; Salter osteotomy.
© 2025 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Wudbhav N Sankar reports a relationship with the Pediatric Orthopaedic Society of North America that includes board membership. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Salter R.B. Role of innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip in the older child. J Bone Joint Surg Am. 1966 Oct;48(7):1413–1439. - PubMed
-
- Bohm P., Brzuske A. Salter innominate osteotomy for the treatment of developmental dysplasia of the hip in children: results of seventy-three consecutive osteotomies after twenty-six to thirty-five years of follow-up. J Bone Joint Surg Am. 2002 Feb;84(2):178–186. - PubMed
-
- Salter R.B. The classic Innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. J Bone Joint Surg Br. 1961;43B(3):518. - PubMed
-
- Salter R.B., Dubos J.P. The first fifteen year's personal experience with innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. Clin Orthop Relat Res. 1974 Jan-Feb;98:72–103. - PubMed
-
- Thomas S.R., Wedge J.H., Salter R.B. Outcome at forty-five years after open reduction and innominate osteotomy for late-presenting developmental dislocation of the hip. J Bone Joint Surg Am. 2007 Nov;89(11):2341–2350. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
