

Time-dependent impact of immunosuppressant regimens on cardiovascular outcomes in kidney transplant recipients: a nationwide cohort study
- PMID: 40432895
- PMCID: PMC12106356
- DOI: 10.3389/fphar.2025.1540576
Time-dependent impact of immunosuppressant regimens on cardiovascular outcomes in kidney transplant recipients: a nationwide cohort study
Abstract
Objectives: We aimed to evaluate the effect of different immunosuppressive regimens on the risk of major adverse cardiovascular events (MACEs) in kidney transplant recipients (KTRs).
Methods: This retrospective cohort study used nationwide claims data from the Korean Health Insurance Review and Assessment Service from between 2010 and 2021. Immunosuppressive medications were analyzed as time-dependent variables, and the primary outcome was MACEs, defined as a composite of myocardial infarction, coronary revascularization, ischemic stroke, and all-cause mortality.
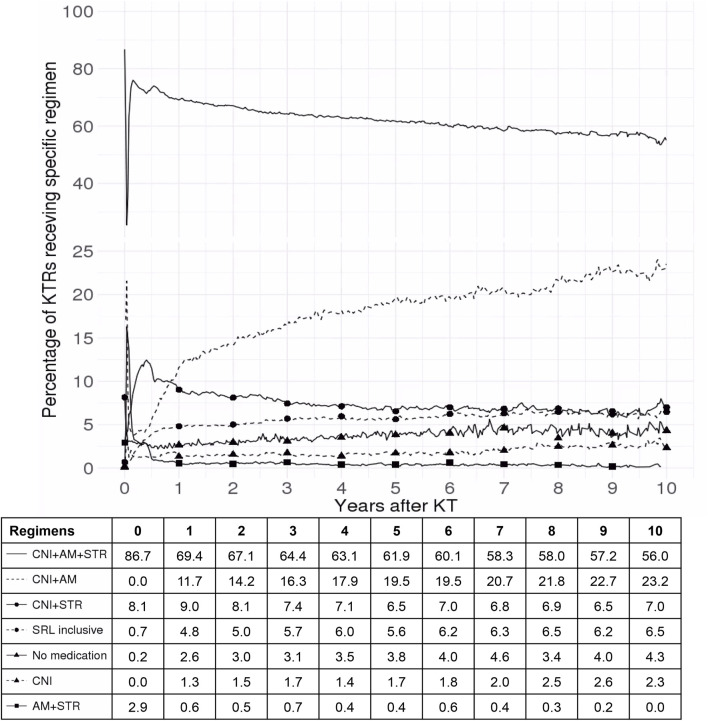
Results: A total of 8,056 KTRs were included in the analysis, with significant risk factors for MACEs identified as male sex, older age, longer dialysis duration, lower economic status, and greater comorbidity. At the time of the kidney transplant, 86.7% of the KTRs were administered standard triple therapy, after which various immunosuppressive regimens, including sirolimus-inclusive regimens, were employed. The risk of MACE was lower or comparable in KTRs standard triple therapy than in those receiving most other immunosuppressive regimens. However, corticosteroid withdrawal was associated with a significant reduction in cardiovascular risk, particularly in KTRs with preexisting diabetes or dyslipidemia.
Conclusion: These findings suggest that early consideration should be given to minimizing steroid use in KTRs with dyslipidemia or diabetes to optimize cardiovascular outcomes.
Keywords: cardiovascular outcomes; comorbidity; immunosuppressive agents; kidney transplantation; time-dependent analysis.
Copyright © 2025 Park, Choi, Hwang, Ah, Chung and Song.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




Similar articles
-
De novo major cardiovascular events in kidney transplant recipients: a comparative matched cohort study.Nephrol Dial Transplant. 2023 Feb 13;38(2):499-506. doi: 10.1093/ndt/gfac144. Nephrol Dial Transplant. 2023. PMID: 35396847
-
Impact of sirolimus on long-term adverse cardiovascular outcomes in kidney transplant recipients: A nationwide cohort study.Eur J Clin Invest. 2025 Jul;55(7):e70027. doi: 10.1111/eci.70027. Epub 2025 Mar 19. Eur J Clin Invest. 2025. PMID: 40105194 Free PMC article.
-
Cardiovascular Outcomes in De Novo Kidney Transplant Recipients Receiving Everolimus and Reduced Calcineurin Inhibitor or Standard Triple Therapy: 24-month Post Hoc Analysis From TRANSFORM Study.Transplantation. 2023 Jul 1;107(7):1593-1604. doi: 10.1097/TP.0000000000004555. Epub 2023 Jun 20. Transplantation. 2023. PMID: 36959121
-
Importance of vascular calcification in kidney transplant recipients.Am J Nephrol. 2014;39(5):418-26. doi: 10.1159/000362492. Epub 2014 May 7. Am J Nephrol. 2014. PMID: 24819032 Review.
-
Target of rapamycin inhibitors (TOR-I; sirolimus and everolimus) for primary immunosuppression in kidney transplant recipients.Cochrane Database Syst Rev. 2019 Dec 16;12(12):CD004290. doi: 10.1002/14651858.CD004290.pub3. Cochrane Database Syst Rev. 2019. PMID: 31840244 Free PMC article.
References
-
- Chen Y.-J., Liu S.-C., Lai K.-L., Tang K.-T., Lin C.-H., Chen Y.-M., et al. (2021). Factors associated with risk of major adverse cardiovascular events in patients with rheumatoid arthritis: a nationwide, population-based, case-control study. Ther. Adv. Musculoskelet. Dis. 13, 1759720X211030809. 10.1177/1759720X211030809 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources