

Enhanced early rehabilitation and pain management with all-arthroscopic medial patellofemoral ligament reconstruction: A comparative study
- PMID: 40433048
- PMCID: PMC12107108
- DOI: 10.1002/jeo2.70291
Enhanced early rehabilitation and pain management with all-arthroscopic medial patellofemoral ligament reconstruction: A comparative study
Abstract
Purpose: The purpose of this study was to evaluate the accuracy of femoral tunnel location, post-operative pain management, functional rehabilitation and clinical outcomes in medial patellofemoral ligament (MPFL) reconstruction using all-arthroscopic technique.
Methods: Between 2020 and 2021, 160 patients with recurrent patellar dislocation undergoing MPFL reconstruction were categorized into control (traditional surgery) and study (all-arthroscopic technique) groups. Femoral tunnel accuracy was assessed via computed tomography scans, pain management, functional rehabilitation, knee range of motion and daily activities were evaluated up to 6 months post-operatively. Knee function was assessed using Kujala and Lysholm scores at post-operative 12 months.
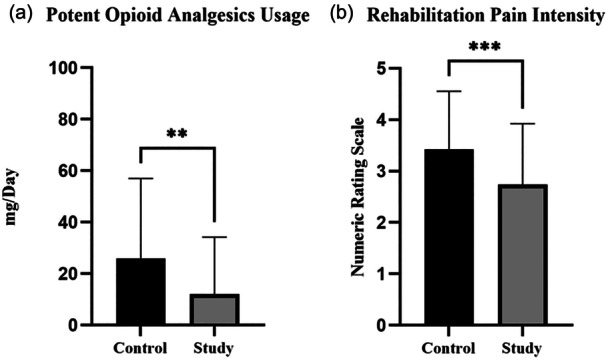
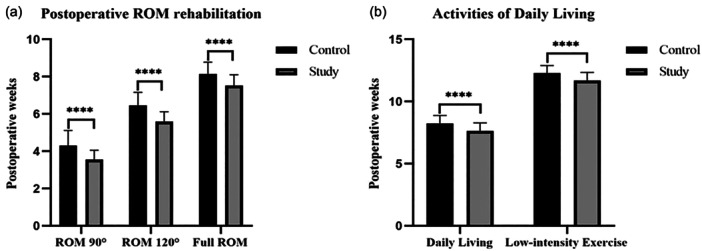
Results: Seventy-one patients in the control group and 69 patients in the study group reached the final follow-up with no demographic differences. Follow-up duration was 12.65 ± 0.68 vs 12.77 ± 0.73 months in the control and study groups (p = 0.3145). The intra-class correlation coefficient was excellent (r = 0.97). In femoral tunnels, 93.5% in the control group and 92.4% in the study group were correctly localized. In patellar tunnels, 96.1% in the control group and 96.2% in the study group were correctly localized (p > 0.9999). Post-operative strong opioid analgesics were used 25.9 ± 31.0 versus 12.0 ± 22.2 mg/day in the control and study groups (p = 0.0016). The pain score was 3.4 ± 1.1 versus 2.7 ± 1.2 in the control and study groups (p = 0.0006) during post-operative functional rehabilitation. Time to resume daily living was 8.2 ± 0.6 versus 7.6 ± 0.6 weeks in the control and study groups (p < 0.0001). Time to resume low-intensity exercise was 12.3 ± 0.6 versus 11.7 ± 0.6 weeks in the control and study groups (p < 0.0001). In the more than 1-year follow-up, no significant difference was found in the Kujala and Lysholm scores.
Conclusions: The all-arthroscopic technique for MPFL reconstruction in recurrent patellar dislocation ensures precise femoral tunnel placement. It offers advantages in early post-operative pain management and functional recovery, enabling faster rehabilitation compared to traditional non-all-arthroscopic techniques.
Level of evidence: Level III.
Keywords: arthroscopy; dislocation; knee; patellar.
© 2025 The Author(s). Journal of Experimental Orthopaedics published by John Wiley & Sons Ltd on behalf of European Society of Sports Traumatology, Knee Surgery and Arthroscopy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
The Effects of Inaccurate Femoral Tunnel Placement During Medial Patellofemoral Ligament Reconstruction on Midterm Clinical Outcomes in Treatment of Recurrent Patellar Dislocation.Am J Sports Med. 2025 Feb;53(2):360-371. doi: 10.1177/03635465241303514. Epub 2025 Jan 4. Am J Sports Med. 2025. PMID: 39754416
-
Does degree of trochlear dysplasia and position of femoral tunnel influence outcome after medial patellofemoral ligament reconstruction?Am J Sports Med. 2014 Mar;42(3):716-22. doi: 10.1177/0363546513518413. Epub 2014 Jan 23. Am J Sports Med. 2014. PMID: 24458241
-
[Optimization location of femoral attachment in medial patellofemoral ligament reconstruction assisted with arthroscopy for patellar dislocation].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020 Oct 15;34(10):1233-1237. doi: 10.7507/1002-1892.202003050. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020. PMID: 33063485 Free PMC article. Chinese.
-
Patellar fixation graft via suture anchors versus tunnel techniques during isolated MPFL reconstruction for recurrent patellofemoral instability: a systematic review of the literature.Arch Orthop Trauma Surg. 2020 Sep;140(9):1201-1210. doi: 10.1007/s00402-020-03420-8. Epub 2020 Apr 21. Arch Orthop Trauma Surg. 2020. PMID: 32318817 Free PMC article.
-
Inconsistencies in Reporting Risk Factors for Medial Patellofemoral Ligament Reconstruction Failure: A Systematic Review.Am J Sports Med. 2022 Mar;50(3):867-877. doi: 10.1177/03635465211003342. Epub 2021 Apr 29. Am J Sports Med. 2022. PMID: 33914648
References
-
- Allahabadi S, Pandya NK. Allograft medial patellofemoral ligament reconstruction in adolescent patients results in a low recurrence rate of patellar dislocation or subluxation at midterm follow‐up. Arthroscopy. 2022;38:128–138. - PubMed
-
- Amis AA, Firer P, Mountney J, Senavongse W, Thomas NP. Anatomy and biomechanics of the medial patellofemoral ligament. Knee. 2003;10:215–220. - PubMed
-
- Balcarek P, Walde TA. Accuracy of femoral tunnel placement in medial patellofemoral ligament reconstruction: the effect of a nearly true‐lateral fluoroscopic view. Am J Sports Med. 2015;43:2228–2232. - PubMed
-
- Cheuy VA, Foran JRH, Paxton RJ, Bade MJ, Zeni JA, Stevens‐Lapsley JE. Arthrofibrosis associated with total knee arthroplasty. J Arthroplasty. 2017;32:2604–2611. - PubMed
-
- Dejour H, Walch G, Nove‐Josserand L, Guier C. Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc. 1994;2:19–26. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
