

Best Practices for Orthopaedic Treatment of Pediatric Gunshot Injuries
- PMID: 40433339
- PMCID: PMC12088179
- DOI: 10.55275/JPOSNA-2023-683
Best Practices for Orthopaedic Treatment of Pediatric Gunshot Injuries
Abstract
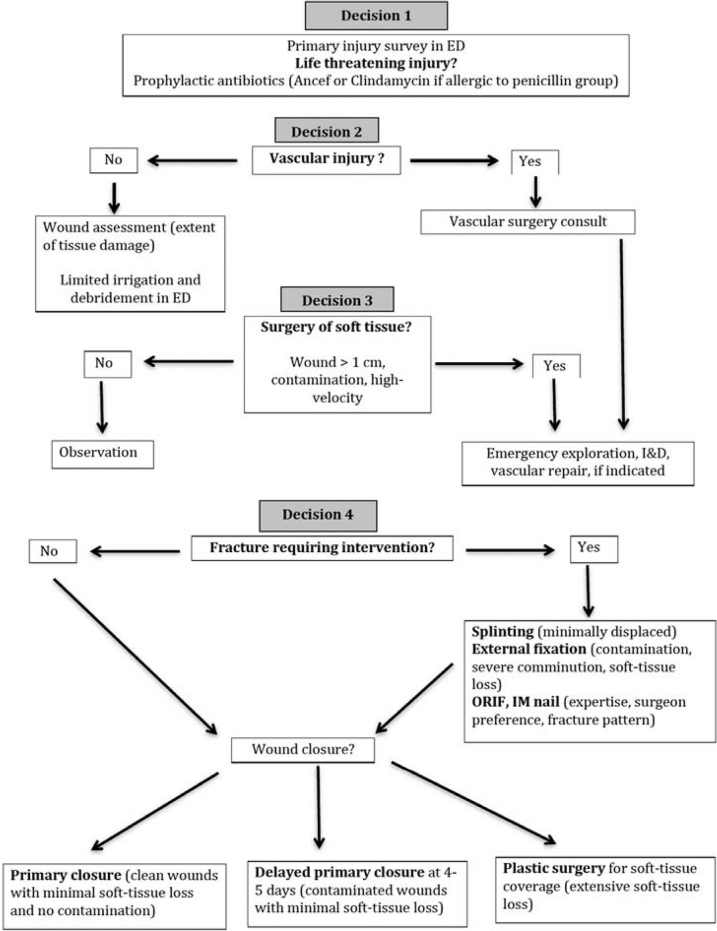
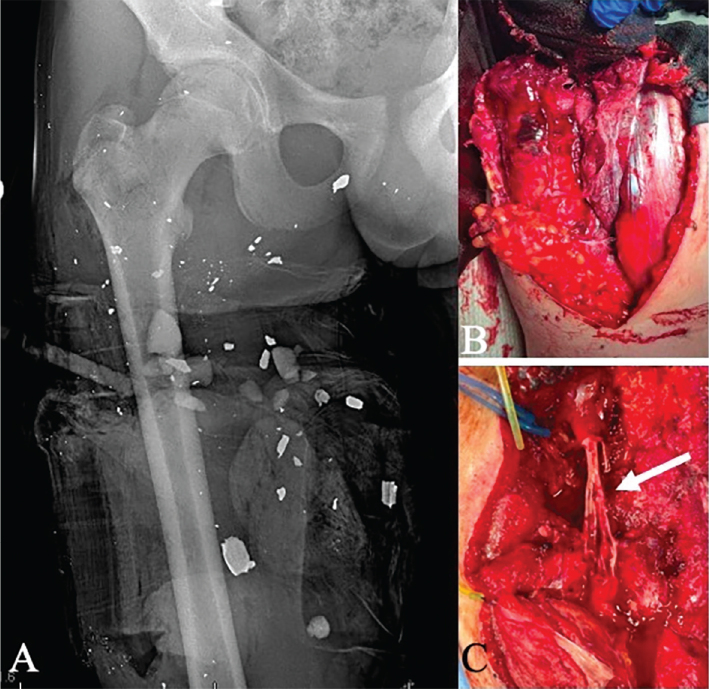
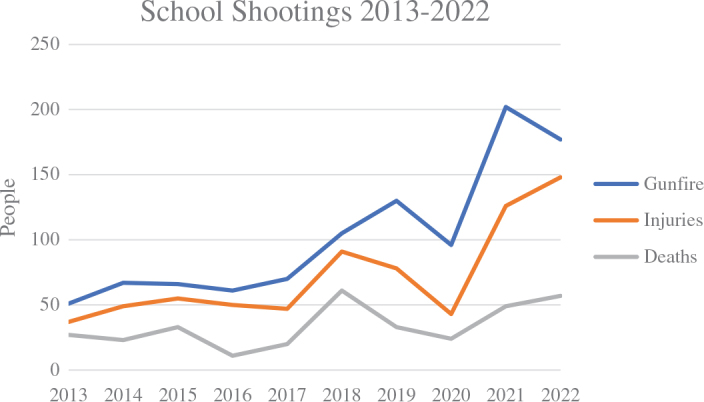
Gun injuries arise from increased access to firearms across the U.S. More firearm injuries are presenting to emergency departments and non-trauma centers. Most are treated with antibiotics, bedside I&D, and non-operative stabilization for simple wounds of <1 cm without contamination and stable fracture patterns. More complex injuries (usually caused by high-velocity weapons) with larger soft tissue defects with contamination, bone loss, operative fracture patterns, intraarticular projectiles, vascular injuries, compartment syndromes, and nerve injuries warrant IV antibiotics and further treatment in the operating room. Only 28% of nerve injuries regain function. Loss to follow-up is high (43%). Growth arrest and lead toxicity are long-term sequelae that must be monitored-the new CDC acceptable blood lead level is <3.5 μg/dL. Gun injuries are now the leading cause of death in children. Evaluation of the child's environment and access to guns and education is important for preventing future injuries on an individual level; however, research and legislation are needed to decrease this epidemic of gun violence injuring and killing children today.
Key concepts: •Gun injuries are currently the leading cause of death in children.•Gun injuries with minimal soft tissue damage and contamination can be treated in the emergency room with bedside debridement, oral antibiotics, and splinting.•Gun injuries with large soft tissue defects, contamination, bone loss, operative fracture patterns, intraarticular projectiles, vascular injuries, compartment syndromes, and nerve injuries warrant further treatment in the operating room and IV antibiotics.•Children with gun injuries involving the physis should be followed for growth arrests and those with retained bullet fragments close to bone or joints for lead toxicity.•Education, research, and legislation are necessary to protect children from gun injuries.
© 2023 JPOSNA. Published by Elsevier on behalf of the Pediatric Orthopaedic Society of North America.
Figures



References
-
- Bleyer A., Siegel S.E., Thomas C.R., Jr. Increasing rate of unintentional firearm deaths in youngest Americans: firearm prevalence and Covid-19 pandemic implication. J Natl Med Assoc. 2021;113(3):265–277. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
