

Efficacy and safety of CD19 combined with CD22 or CD20 chimeric antigen receptor T-cell therapy for hematological malignancies
- PMID: 40433368
- PMCID: PMC12106392
- DOI: 10.3389/fimmu.2025.1577360
Efficacy and safety of CD19 combined with CD22 or CD20 chimeric antigen receptor T-cell therapy for hematological malignancies
Abstract
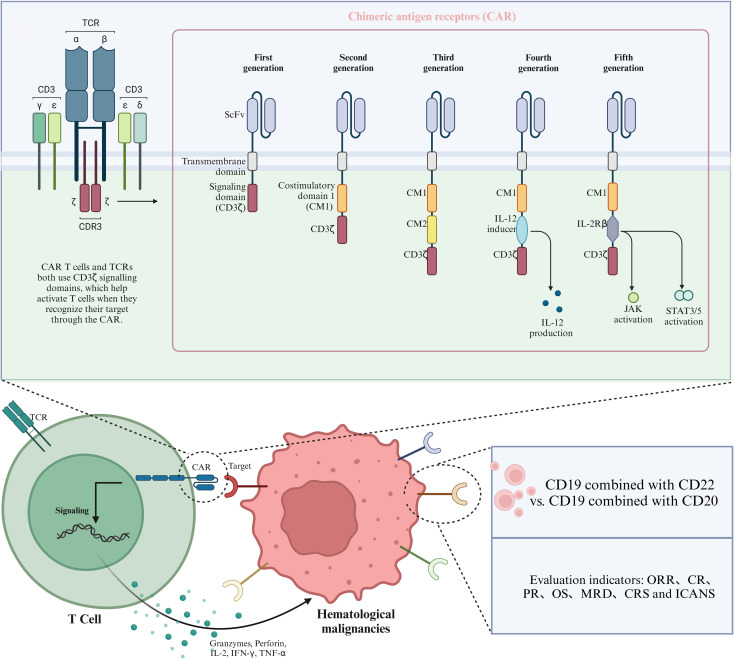
Background: CD19 combined with CD22 or CD20 therapy is a promising immunotherapy approach for the treatment of hematological malignancies. Dual-targeted CD19/CD22 CAR T and CD19/CD22 CAR T-cell therapy are currently being evaluated in clinical trials, and the extent of improvement using CD19 in combination with dual-targeted therapy has not yet been determined. To compare the differences between the two in the treatment of hematological tumors, this study summarized the available evidence. To evaluate and compare the efficacy and safety of CD19-combined CD22 and CD19-combined CD20 CAR T-cell therapy.
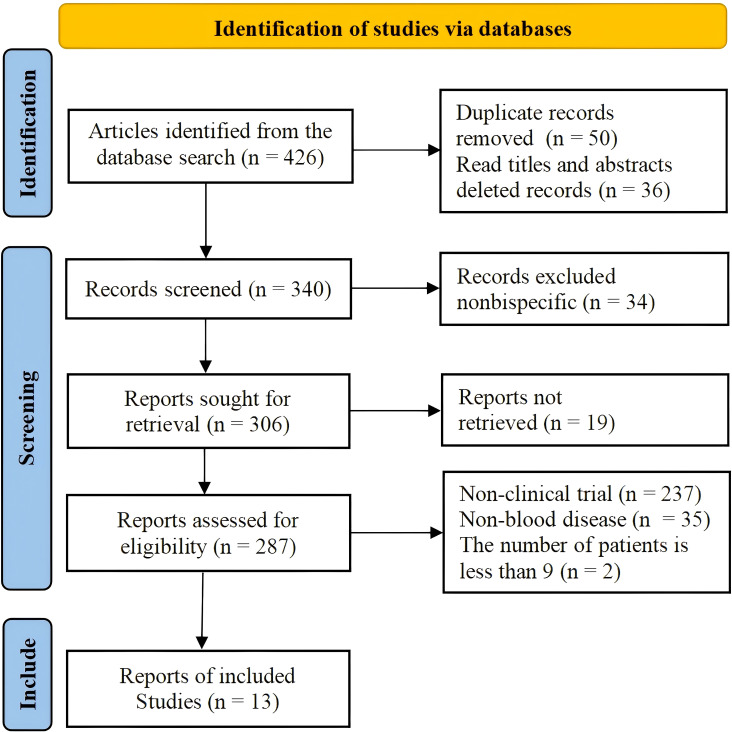
Methods: Data from 13 clinical studies that included 628 patients with hematological malignancies were extracted and analyzed based on a set of inclusion and exclusion criteria. The primary efficacy outcomes were overall response rate (ORR), complete response (CR) rate, partial response (PR) rate, overall survival (OS) rate and minimal residual disease (MRD)-negative response rate. The safety outcomes were cytokine release syndrome (CRS) rate and immune effector cell-associated neurotoxicity syndrome (ICANS) rate.
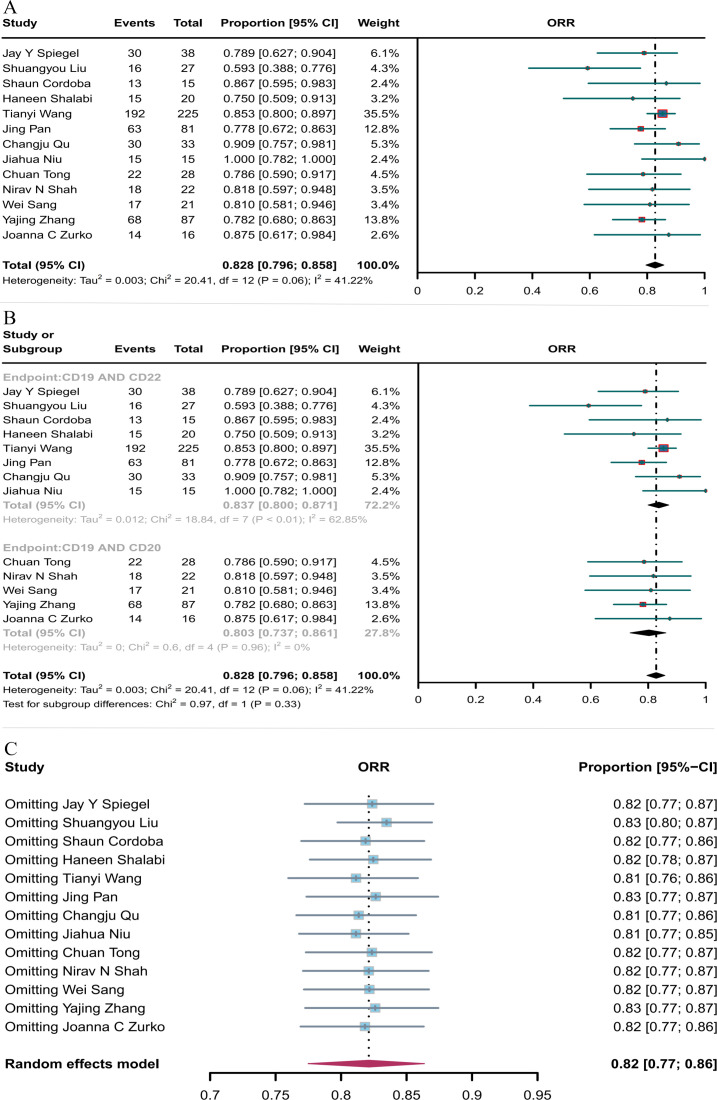
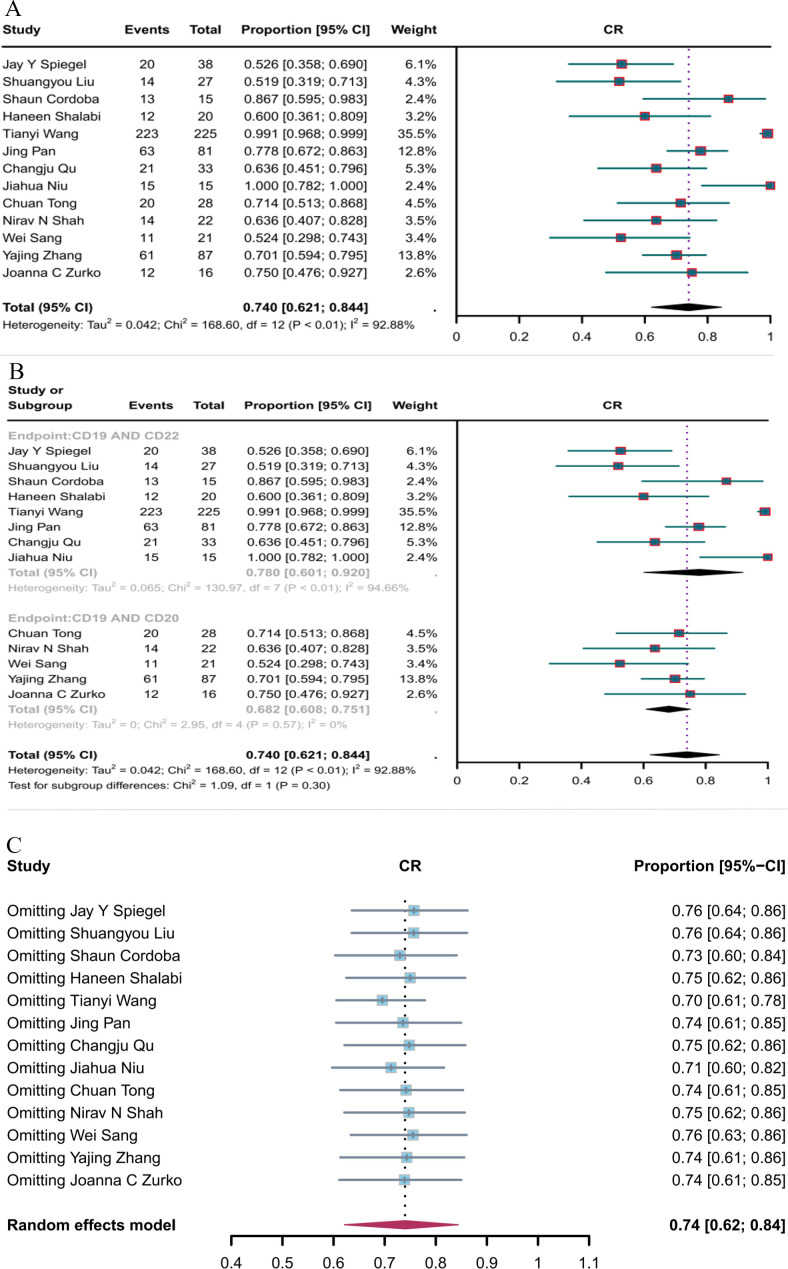
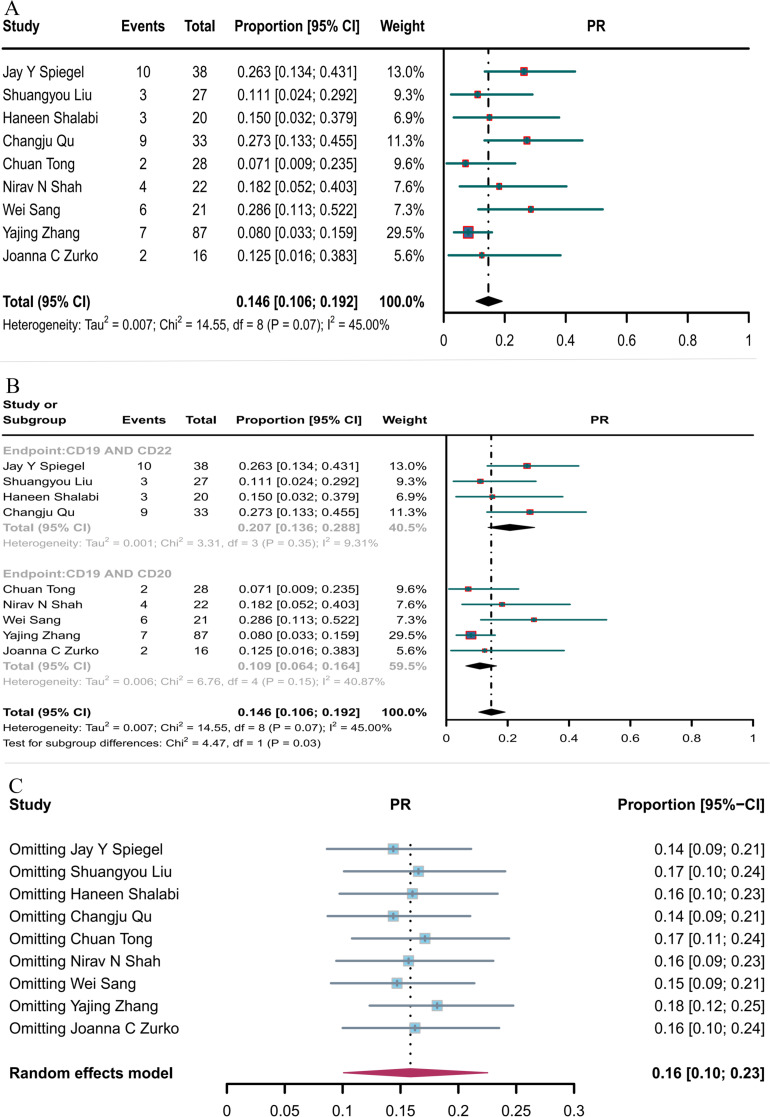
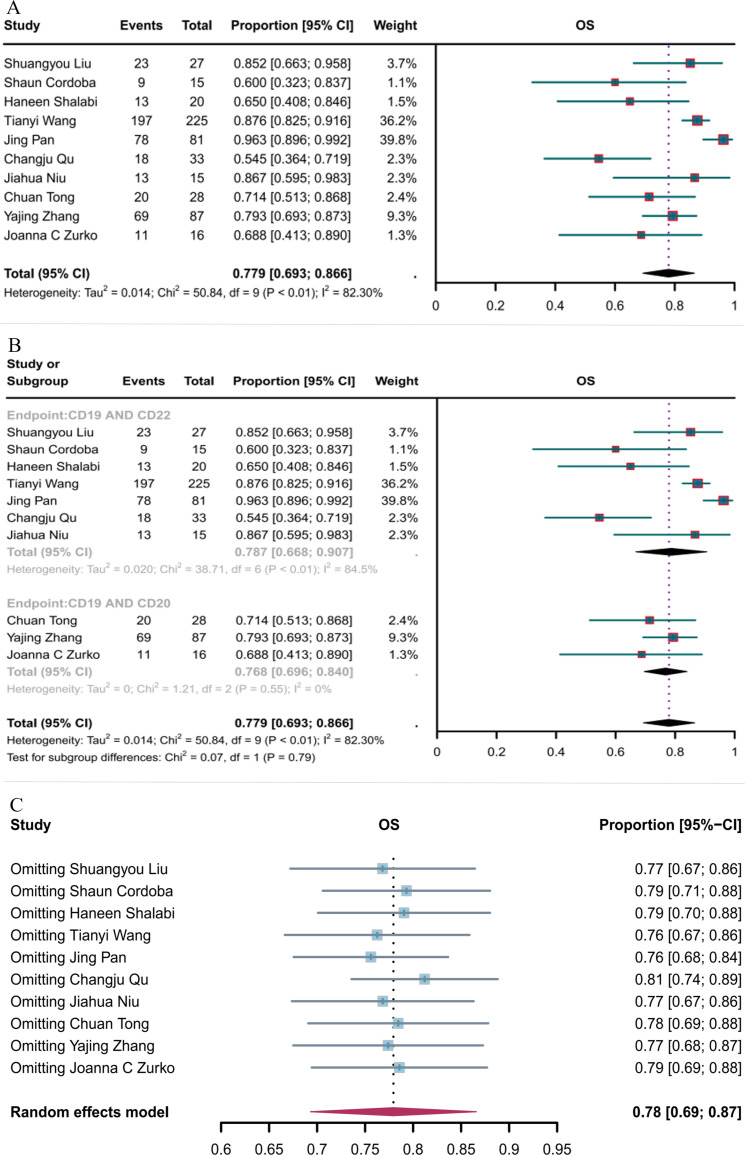
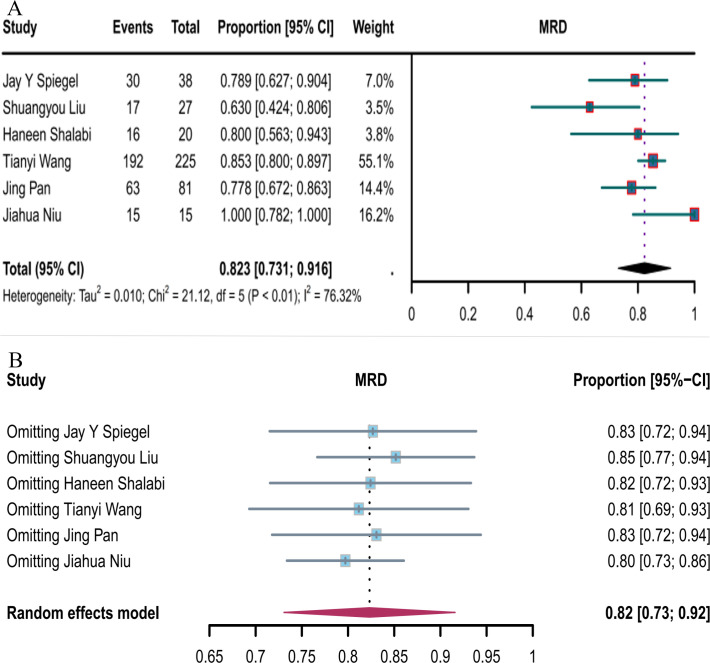
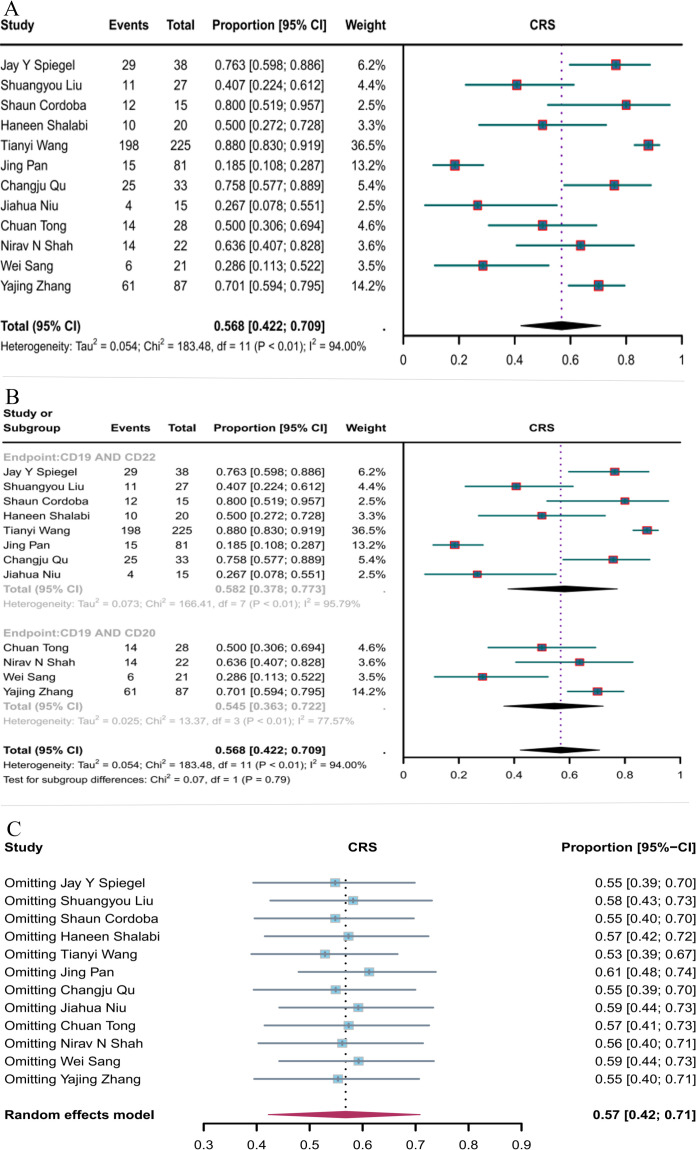
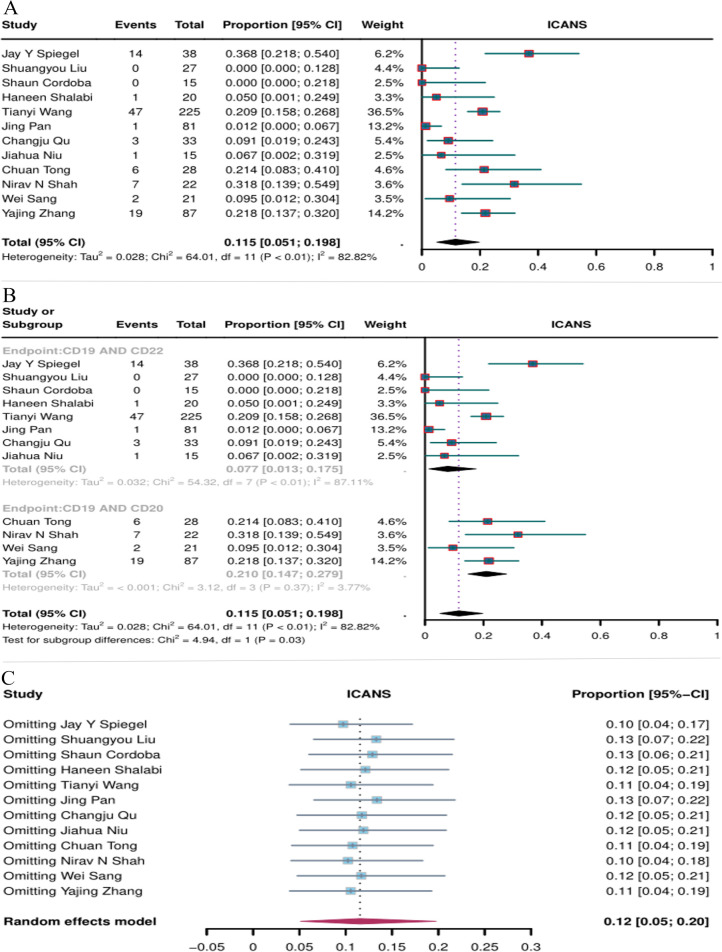
Results: For CD19 combined with CD22 CAR T-cell therapy, the ORR was 83.7%; CR, 78.0%; PR, 20.7%, OS, 78.7%; MRD-negative response rate, 82.3%; incidence of CRS, 58.2%; ICANS, 7.7%. For CD19 combined with CD20 CAR T-cell therapy, the ORR was 80.3%; CR, 68.2%; PR, 10.9%; OS, 76.8%; incidence of CRS, 54.5%; ICANS, 21%. Subgroup analysis indicated that the PR of CD19 combined with CD22 was significantly greater than that of CD19 combined with CD20, and the incidence of ICANS was significantly lower with the CD19+CD22 CAR-T combination.
Conclusion: The data from this study suggest that CD19 combined with CD22 CAR T-cell therapy had a higher partial response rate in the treatment of hematologic malignancies and higher safety profile in the occurrence of ICANS than CD19 combined with CD20. These data provide an important clinical basis for the development of new therapeutic targets and the construction of therapeutic methods for the treatment of hematologic malignancies, and broaden our understanding of CD19 dual-targeted CAR T therapy.
Keywords: cancer therapy; car-t; chimeric antigen receptor; hematological malignancies; immunotherapy.
Copyright © 2025 Yuan, Wang, Zhao, Yang, Yang, Tian, Li, Liu, Wang, Tang, He, Li and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials