

Oncogenomic profiling in infant-toddler T-ALL identifies NKX2 family genes as drivers linked to favorable outcomes
- PMID: 40433554
- PMCID: PMC12108104
- DOI: 10.1002/hem3.70154
Oncogenomic profiling in infant-toddler T-ALL identifies NKX2 family genes as drivers linked to favorable outcomes
Abstract
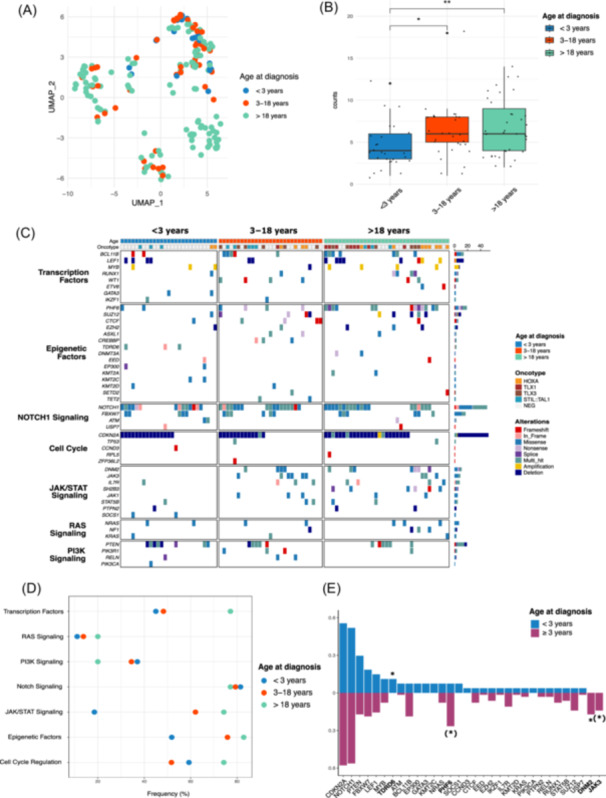
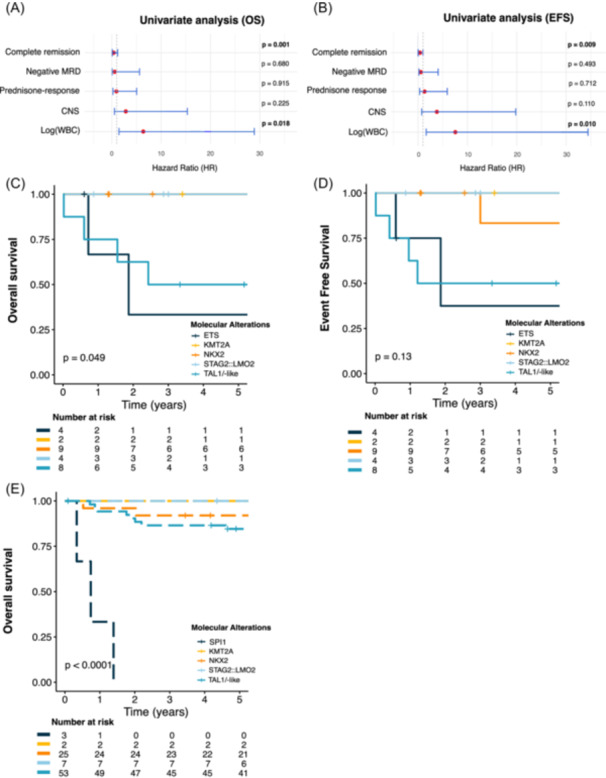
T-cell acute lymphoblastic leukemia (T-ALL) is a rare and aggressive hematological malignancy primarily affecting adolescents and young adults and is scarce in infants and toddlers under age 3. Unlike B-ALL, T-ALL in this young population remains poorly characterized due to limited data and lacks evidence-based guidelines to help clinicians determine the optimal treatment approach. In this study, we conducted a comprehensive genetic analysis of infant/toddler T-ALL cases from a French national cohort, utilizing high-throughput targeted sequencing, optical genome mapping, and RNA sequencing. Genetic analysis revealed the absence of TLX1/3 dysregulation. Instead, we identified a significant prevalence of NKX2 rearrangements (n = 9, 33%), co-occurring with MYB alterations (n = 5/9) or chromothripsis-like events (n = 3/9). Additional findings included TAL1/-like anomalies (30%), STAG2::LMO2 (15%), ETS rearrangements (15%), and rarely, KMT2A rearrangements (7%). Comparative analyses with 245 patients aged 3-18 years, enrolled in the pediatric FRALLE2000T French protocol, underscored the distinct clinical and genetic profiles of infants/toddlers. Despite presenting with higher rates of hyperleukocytosis and slower responses to treatment, they demonstrated comparable survival outcomes to older pediatric patients, with a 5-year overall survival (OS) rate of 75.4% (95% confidence interval [CI]: 60.0%-94.8%) versus 75.2% (95% CI: 69.8%-81.1%), p = 0.86. Notably, alterations in NKX2, KMT2A, and STAG2::LMO2 delineated oncogenic subgroups exhibiting a remarkable 100% OS rate, while patients with TAL1 or ETS dysregulation experienced less favorable outcomes. This was further supported by analyses of data from the COG AALL0434 trial, enhancing our understanding of T-ALL in infants/toddlers. Large-scale collaborative studies remain essential to confirm these findings and refine treatment strategies.
© 2025 The Author(s). HemaSphere published by John Wiley & Sons Ltd on behalf of European Hematology Association.
Conflict of interest statement
The authors declare no competing financial interests.
Figures


References
-
- Asnafi V, Beldjord K, Boulanger E, et al. Analysis of TCR, pTα, and RAG‐1 in T‐acute lymphoblastic leukemias improves understanding of early human T‐lymphoid lineage commitment. Blood. 2003;101:2693‐2703. - PubMed
-
- Clappier E, Cuccuini W, Kalota A, et al. The C‐MYB locus is involved in chromosomal translocation and genomic duplications in human T‐cell acute leukemia (T‐ALL), the translocation defining a new T‐ALL subtype in very young children. Blood. 2007;110:1251‐1261. - PubMed
-
- Stutterheim J, de Lorenzo P, van der Sluis IM, et al. Minimal residual disease and outcome characteristics in infant KMT2A‐germline acute lymphoblastic leukaemia treated on the Interfant‐06 protocol. Eur J Cancer. 2022;160:72‐79. - PubMed
-
- Asnafi V, Beldjord K, Libura M, et al. Age‐related phenotypic and oncogenic differences in T‐cell acute lymphoblastic leukemias may reflect thymic atrophy. Blood. 2004;104:4173‐4180. - PubMed
LinkOut - more resources
Full Text Sources