

Association of cardiometabolic multimorbidity with postoperative delirium and three-year mortality in patients undergoing knee/hip arthroplasty: a prospective cohort study
- PMID: 40434729
- PMCID: PMC12165473
- DOI: 10.1097/JS9.0000000000002379
Association of cardiometabolic multimorbidity with postoperative delirium and three-year mortality in patients undergoing knee/hip arthroplasty: a prospective cohort study
Abstract
Introduction: Postoperative delirium (POD) is a severe and common complication. This study aimed to investigate the association of cardiometabolic multimorbidity (CMM) and their different subgroups with POD.
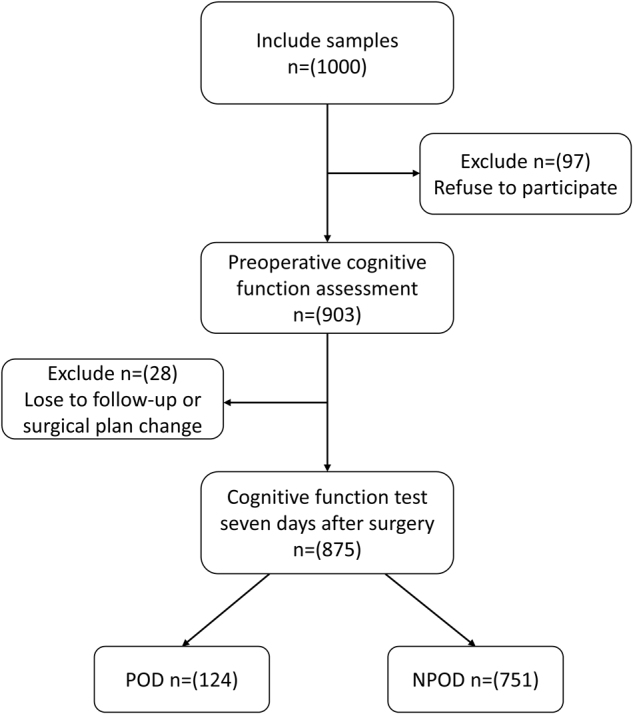
Methods: This prospective cohort study ultimately included 875 patient samples from the Perioperative Neurocognitive Disorder and Lifestyle Biomarkers (PNDABLE) database, collected between July 2020 and September 2021. In this study, patients were first categorized into a POD group and a non-POD group, and the demographic characteristics of the two groups were compared. Next, logistic regression models were used to analyze the association between CMM and POD, as well as between cerebrospinal fluid (CSF) biomarkers and POD. Additionally, the models examined the relationship between different CMM subtypes and the incidence of POD. Subsequently, the robustness of the results was verified by sensitivity analysis and post hoc analysis. Further, the role of CSF biomarkers in the relationship between CMM and POD was assessed using mediation analysis. Finally, CMM patients with POD were followed up for three years, and Kaplan-Meier (K-M) survival analysis was used to compare the mortality rates of different CMM subgroups in patients with POD.
Results: Logistic regression analysis showed that CMM [odds ratio: 5.062; 95% CI: 3.279-7.661; P < 0.001], T-tau, and P-tau were risk factors for POD, while Aβ42 was a protective factor. Associations between different CMM subgroups and POD varied. Sensitivity and post hoc analyses supported these findings. Mediation analysis indicated that CMM could increase the incidence of POD through the CSF T-tau (proportion: 11%, P < 0.050). A follow-up of 50 patients showed that K-M survival analysis revealed that the POD patients in the diabetes combined with coronary heart disease group had a significantly higher three-year mortality compared to other CMM subgroups ( P = 0.004).
Conclusions: CMM may be a risk factor for POD, with CSF T-tau potentially playing a mediating role. These findings underscore the importance of preoperative cognitive assessment for risk stratification and suggest CSF T-tau as a potential intervention target. Future studies may further explore intervention strategies targeting CMM and CSF T-tau.
Keywords: anesthesiology; cardiometabolic multimorbidity; cerebrospinal fluid; cohort study; delirium; neuropsychological tests; postoperative delirium.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
None.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
