

Association of Self-Reported Sleep Metrics With Imaging Markers of Small Vessel Disease and Cognition in Patients With TIA or Mild Stroke
- PMID: 40435444
- PMCID: PMC12113490
- DOI: 10.1212/WNL.0000000000213734
Association of Self-Reported Sleep Metrics With Imaging Markers of Small Vessel Disease and Cognition in Patients With TIA or Mild Stroke
Abstract
Background and objectives: Disturbed sleep is common after stroke, yet its relationship with cerebral small vessel disease (SVD) and cognitive performance in the stroke population, particularly patients with TIA/mild stroke who are on the milder end of the cerebrovascular spectrum, remains understudied. We aim to examine the associations of self-reported sleep metrics with neuroimaging markers of SVD and cognitive performance in patients with TIA/mild stroke from 2 prospective stroke cohorts.
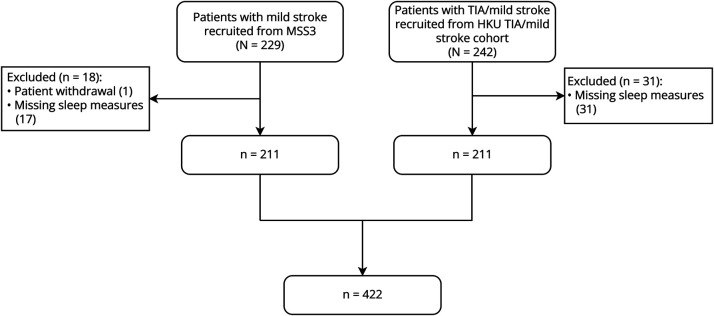
Methods: We studied adult patients with TIA/mild stroke (NIH Stroke Scale [NIHSS] score <7) who were consecutively recruited from Mild Stroke Study 3 (MSS3, University of Edinburgh) and the stroke cohort (the University of Hong Kong, HKU) during 2018-2022. Both MSS3 (N = 211) and HKU (N = 211) cohorts assessed SVD burden visually on brain MRI, cognitive performance using Montreal Cognitive Assessment (MoCA), and sleep quality using a structured sleep questionnaire at baseline visit. The primary outcomes were SVD markers, and the secondary outcome was total MoCA score. The associations of sleep metrics with SVD markers and cognitive performance were assessed using regression models, adjusted for demographics, vascular risk factors, history of depression and stroke, and study sites.
Results: In 422 patients (65.6 ± 11.8 years, 67% male, median NIHSS score 1.0), longer in-bed time was independently associated with greater global SVD and Fazekas periventricular white matter hyperintensity (WMH) burden: odds ratio (OR)summary SVD score = 1.27 per 1-SD increase (95% CI 1.05-1.53), false discovery rate (FDR)-adjusted p = 0.04; ORperiventricular WMH = 1.53 per 1-SD increase (95% CI 1.18-2.00), p = 0.003. Longer sleep duration was independently associated with presence of cerebral microbleeds: OR = 1.42 per 1-SD increase (95% CI 1.09-1.87), p = 0.04. Longer in-bed time was associated with a lower total MoCA score after covariate adjustment: standardized β = -0.58 (95% CI -0.99 to -0.16), p = 0.02.
Discussion: Disturbed sleep, including longer in-bed time and longer sleep duration, was cross-sectionally associated with greater SVD burden and worse cognitive performance in patients with TIA/mild stroke. Future longitudinal studies are warranted to validate our findings.
Conflict of interest statement
The authors report no relevant disclosures. Go to
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical