

Recent Pathophysiological Insights Are Advancing the Treatment of Venous Thromboembolism
- PMID: 40436530
- PMCID: PMC12235317
- DOI: 10.1016/j.jacbts.2024.12.004
Recent Pathophysiological Insights Are Advancing the Treatment of Venous Thromboembolism
Abstract
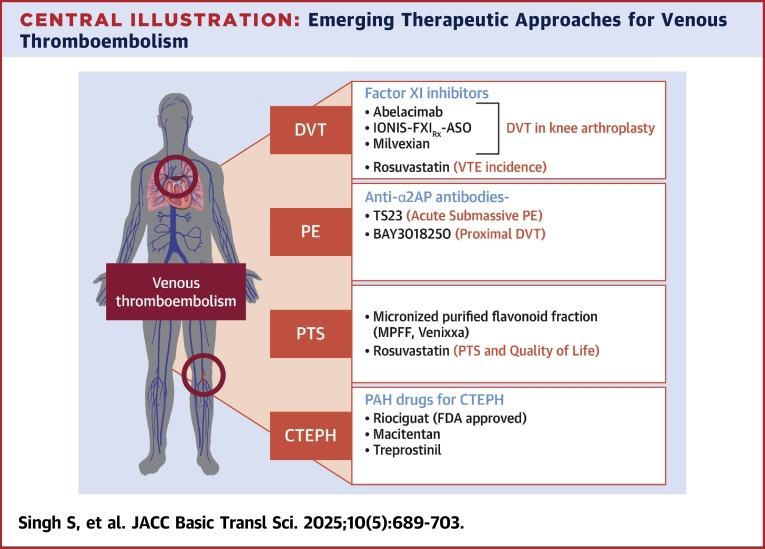
Venous thromboembolism, defined as deep vein thrombosis and pulmonary embolism, is the third leading cause of cardiovascular deaths globally. Long-term complications of unresolved venous thrombi include post-thrombotic syndrome in the legs and chronic thromboembolic pulmonary hypertension. As the venous thrombus ages, the acute, fibrin, and red blood cell-rich composition changes to a chronic cellular, fibrotic mass that does not respond to presently available therapeutic approaches. Standard anticoagulation treatment does not fully prevent recurrent thrombosis and may cause serious bleeding. Thrombolytic therapy may resolve thrombi but it has unacceptable bleeding risks. Recent drug discovery for acute venous thromboembolism has focused on novel targets that may provide enhanced safety and efficacy. Additional therapeutic strategies have focused on the transition phase of acute-to-chronic venous thromboembolism with anti-inflammatory agents, statins, and vasodilator drugs. In this review, we discuss the mechanisms of venous thrombus aging, its clinical implications, and the latest developments in pharmacotherapeutic approaches for venous thromboembolism.
Keywords: CTEPH; Factor XI; PTS; fibrinolysis inhibitors; thrombus composition; venous thromboembolism; venous thrombosis.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was funded in part by the Ramanujan Fellowship (RJF/2020/000070) by SERB-DST, Government of India. Institutional support was provided by CSIR-IHBT Project MLP0204 (Department of Dietetics and Nutrition Technology) to Dr Singh; and National Institutes of Health funding to Dr Reed (HL092750, HL158376) and Dr Jaffer (HL144550, HL150538, HL16543). Dr Jaffer has sponsored research for Canon, Siemens, Shockwave, Teleflex, Mercator, Boston Scientific, HeartFlow, and Neovasc; has received consultant/speaker fees from Boston Scientific, Siemens, Magenta Medical, Philips, Biotronik, Mercator, Terumo, Abiomed, Shockwave, DurVena, Intravascular Imaging Inc, Medtronic, and FastWave; has equity interest in Intravascular Imaging Inc, DurVena, and FastWave; and his institution, Massachusetts General Hospital, has licensing arrangements with Terumo, Canon, and Spectrawave, for which he has the right to receive royalties. Dr Reed is the founder and CSO of Translational Sciences. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures




References
-
- Huisman M.V., Barco S., Cannegieter S.C., et al. Pulmonary embolism. Nat Rev Dis Primers. 2018;4 - PubMed
-
- Wolberg A.S., Rosendaal F.R., Weitz J.I., et al. Venous thrombosis. Nat Rev Dis Primers. 2015;1 - PubMed
-
- Mumoli N., Invernizzi C., Luschi R., et al. Phlegmasia cerulea dolens. Circulation. 2012;125:1056–1057. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
