

Determining the minimum important differences for field walking tests in adults with long-term conditions: a systematic review and meta-analysis
- PMID: 40436612
- PMCID: PMC12117381
- DOI: 10.1183/16000617.0198-2024
Determining the minimum important differences for field walking tests in adults with long-term conditions: a systematic review and meta-analysis
Erratum in
-
"Determining the minimum important differences for field walking tests in adults with long-term conditions: a systematic review and meta-analysis". E. Daynes, R.E. Barker, A.V. Jones, et al. Eur Respir Rev 2025; 34: 240198.Eur Respir Rev. 2025 Jun 18;34(176):245198. doi: 10.1183/16000617.5198-2024. Print 2025 Apr. Eur Respir Rev. 2025. PMID: 40533104 Free PMC article. No abstract available.
Abstract
Importance: The minimum important difference (MID) for field walking tests aims to improve interpretation of outcomes, but the volume and heterogeneity of MIDs for these tests is challenging. We aimed to determine the MID for the 6-min walk distance (6MWD), incremental shuttle walk test (ISWT) and endurance shuttle walk test (ESWT) in adults with long-term conditions.
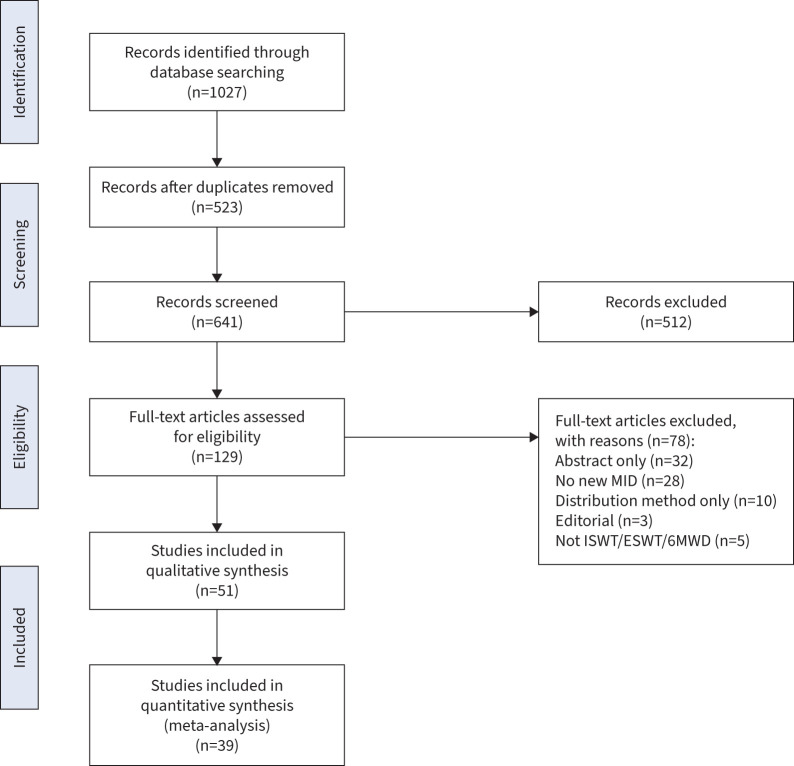
Methods: This systematic review included studies that generated a MID using an anchor-based approach in patients with long-term conditions for the 6MWD, ISWT or ESWT field walking tests. Studies were screened and data extracted by independent reviewers. Meta-analyses were performed using RevMan.
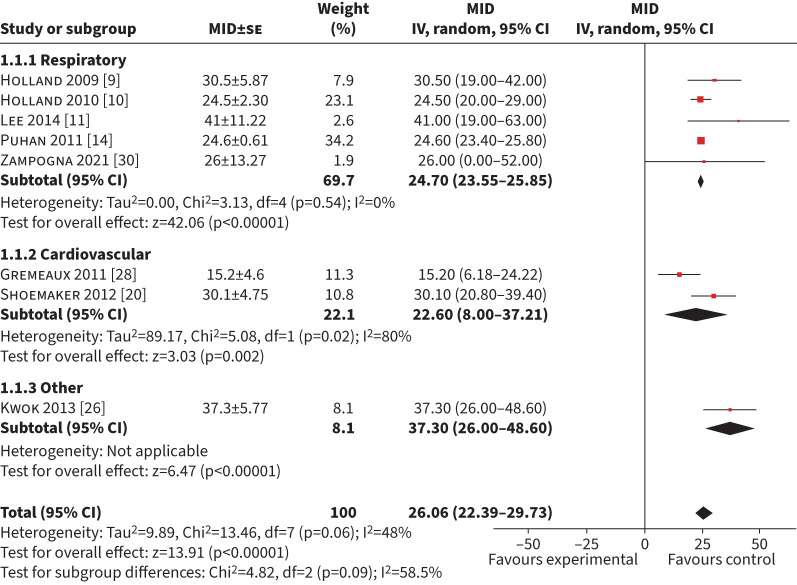
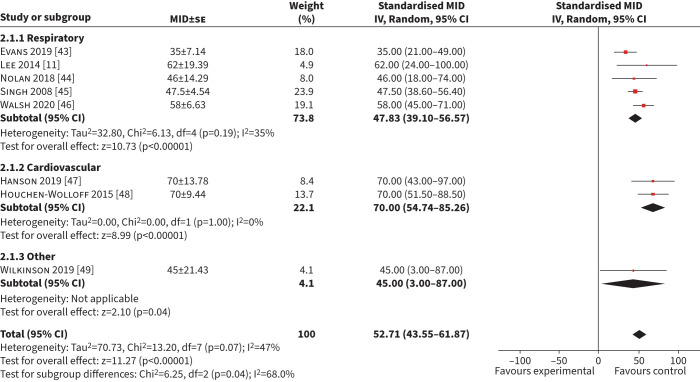
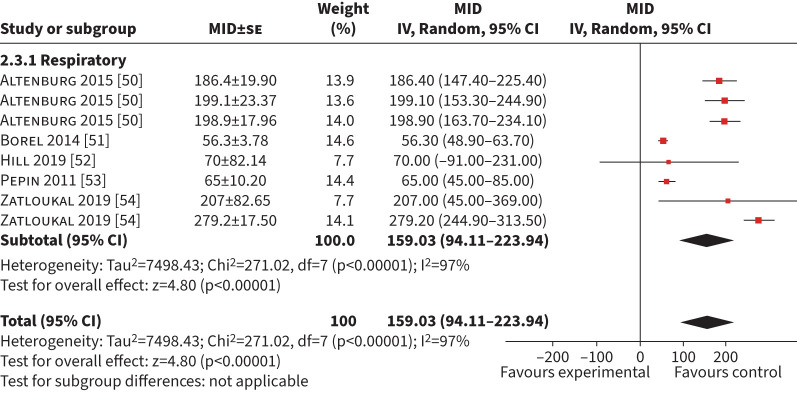
Results: 42 studies were included in the analyses, involving n=13 949 participants. Of these, 12 studies involving exercise as an intervention were included in the meta-analyses to produce MIDs, presented as mean (95% confidence interval). The MID for the 6MWD was 25 m (24-26 m) for respiratory conditions, 23 m (8-37 m) for cardiac conditions and 37 m (26-49 m) for neurological/musculoskeletal conditions. The MID for the ISWT was 48 m (39-57 m) for respiratory conditions and 70 m (55-85 m) for cardiac conditions. The MID for ESWT in COPD was 159 s (94-224 s). The pooled MID across conditions within exercise interventions was 26 m (22-40 m) for the 6MWD and 53 m (44-62 m) for the ISWT, with reasonable heterogeneity (I2=48% and I2=47%, respectively).
Conclusion: We propose new MIDs for exercise interventions using anchor-based methodology in long‑term conditions for the 6MWD, ISWT and ESWT. These can be used internationally for meta‑analyses where studies have used different field walking tests, to optimise trial sample size calculations, and for clinical service benchmarking.
Copyright ©The authors 2025.
Conflict of interest statement
Conflict of interest: E. Daynes reports consulting fees from Neuroscience Mental Health Institute as a Long COVID funding reviewer, payment for lectures from Clinical Physio, and leadership roles with British Thoracic Society Pulmonary Rehabilitation Special Advisory Group and Royal College of Physicians (RCP) Pulmonary Rehabilitation Services Accreditation Scheme Quality Lead. R.E. Barker, A.V. Jones, J.A. Walsh and C.M. Nolan have nothing to disclose. W.D-C. Man reports grants from the National Institute for Health Research and Small Business Research Initiative and a leadership role as Honorary President of the Association for Respiratory Technology and Physiology. S.J. Singh reports grants from National Institute for Health and Care Research (NIHR) Programme Grant (NIHR 202020), Wellcome Doctoral Training Programme, Health Technology Assessment Project Grant (NIHR: 131015), NIHR DHSC/UKRI COVID-19 Rapid Response Initiative, NIHR Global Research Group (NIHR 17/63/20), Actegy Limited and NIHR Senior Investigator; payment or honoraria for lectures, presentations or educational events from GSK, Ministry of Justice, CIPLA and Sherbourne Gibbs; participation on a data safety monitoring board with National Institute for Health and Care Excellence (NICE) Expert Adviser Panel for Long COVID and Wales Long COVID Advisory Board (expired); and leadership roles with American Thoracic Society (ATS) Pulmonary Rehabilitation Assembly Chair, Clinical Lead RCP Pulmonary Rehabilitation Accreditation Scheme, and Clinical Lead National Asthma and COPD Audit Programme for Pulmonary Rehabilitation. N.J. Greening reports grants from GSK, Genentech and Roche; consultancy fees from Genentech and Roche; payment or honoraria for lectures, presentations or educational events from AstraZeneca, Chiesi, GSK and PulmonX; support for attending meetings from Chiesi and AstraZeneca; and participation on a data safety monitoring board with rehabilitation, exercise and supplementation trials in COPD. L. Houchen-Wolloff has nothing to disclose. R.A. Evans reports support for other studies from UK Research and Innovation/Medical Research Council/NIHR; grants from Wolfson Foundation and Genentech/Roche; consulting fees from AstraZeneca/Evidera for Long COVID; payment or honoraria for lectures or presentations from Boehringer and Moderna; support for attending meetings from Chiesi; and unpaid leadership roles with ERS Group 01.02 Pulmonary Rehabilitation and Chronic Care (Secretary) and ATS Pulmonary Rehabilitation Assembly Chair.
Figures
References
-
- Department of Health . Long Term Conditions Compendium of Information. Third Edition. Available from: https://assets.publishing.service.gov.uk/media/5a7c638340f0b62aff6c154e/... Date last updated: 30 May 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical