

Online adaptive stereotactic body radiotherapy for localized prostate cancer in patients with lower urinary tract symptoms and/or prostate hyperplasia (X-SMILE)
- PMID: 40437508
- PMCID: PMC12117833
- DOI: 10.1186/s13014-025-02653-4
Online adaptive stereotactic body radiotherapy for localized prostate cancer in patients with lower urinary tract symptoms and/or prostate hyperplasia (X-SMILE)
Abstract
Background: Stereotactic body radiotherapy (SBRT) for localized prostate cancer offers non-inferior oncological outcomes and toxicity profiles compared to conventionally or moderately hypofractioned radiotherapy regimens, with shorter treatment durations. However, SBRT may not be suitable for all patients, particularly those with lower urogenital tract symptoms and/or prostatic hyperplasia.
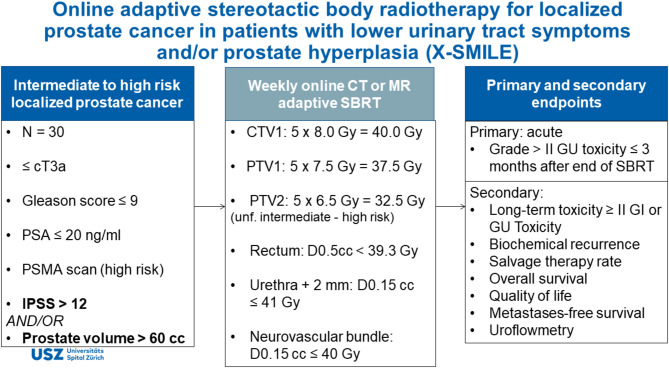
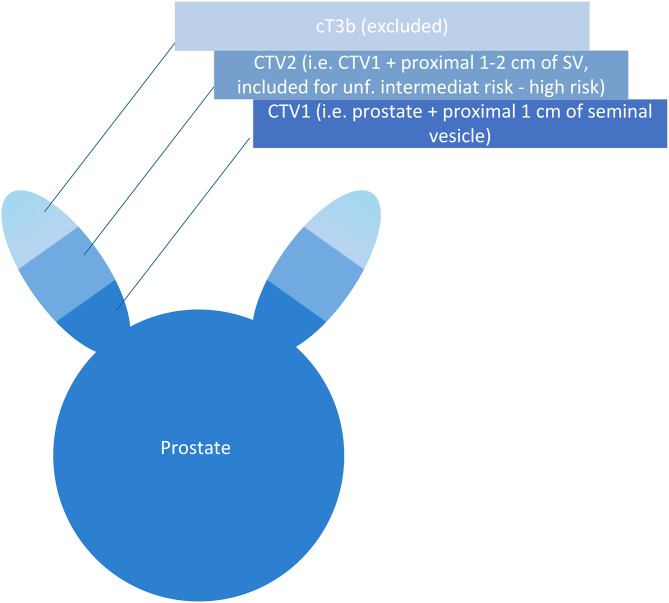
Methods: This study aims to evaluate the safety and efficacy of weekly computed tomography (CT) or magnetic resonance image (MRI)-guided online adaptive SBRT in patients with intermediate to high-risk localized prostate cancer (i.e. ≤ cT3a and Gleason score ≤ 9 and PSA ≤ 20 ng/ml) who present with lower urinary tract symptoms (International Prostate Symptom Score [IPSS] > 12) and/or have prostate hyperplasia (prostate volume > 60 mL). The primary outcome measure is urogenital toxicity grade ≥ 3 within 3 months after completion of SBRT (according to CTCAE V5.0) or treatment-related discontinuation. Our aim is to show an event rate of 3% below a clinically acceptable threshold which is set at 20%. Under the null hypothesis, this design with an alpha of 0.05 and power of 80% results in an expected number of cases of 30.
Discussion: In cases of moderate to high IPSS or significant obstructive urodynamics, a pre-emptive transurethral resection of prostate (TURP) may be beneficial. Notably, 10-20% of prostate cancer patients receiving radiotherapy patients have a history of TURP. While TURP can improve obstructive symptoms, its impact on late toxicity, particularly in SBRT, requires further investigation. To mitigate the risk of urogenital toxicity, especially in the case of patients with lower urogenital tract symptoms and/or prostatic hyperplasia, emerging approaches like MR-guided adaptive SBRT and weekly SBRT have shown promise.
Trial registration: ClinicalTrials.gov/NCT06834152.
Protocol version: Version 6.0.
Keywords: BPH; CT; LUTS; Localized prostate cancer; Lower urogenital tract symptoms; MRI; Prostate cancer; Prostatic hyperplasia; SBRT; Stereotactic radiotherapy.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The final protocol was approved by the Ethics Committee of the University of Zurich, Zurich, Switzerland (Zurich: 2024 − 00115). The X-SMILE study complies with the Helsinki Declaration in its recent German version, the principles of Good Clinical Practice (GCP) and the General Data Protection Regulation (GDPR) as well as the Federal Data Protection Act (FDPA). The trial will also be carried out in accordance with local legal and regulatory requirements. The ClinicalTrials.gov identifier is NCT06834152. Consent for publication: Not applicable. Protocol amendments: Substantial changes to the project set-up, the protocol and relevant project documents will be submitted to the Ethics Committee for approval according to HRO Art. 18 before implementation. Roles and responsibilities: The sponsor had a role in the study design, but not in the collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication. The funder had no role in the study design, collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication. Confidentiality: Project data will be handled with uttermost discretion and is only accessible to authorized personnel who require the data to fulfil their duties within the scope of the research project. On the CRFs and other project specific documents, participants are only identified by a unique participant number. The project site personnel maintain a participant identification list, in which the participant identification numbers are linked to the full participant names and dates of birth. This list will be kept strictly confidential and must not leave the project site. After completion of the project, the participant identification list will be archived for 15 years. All clinical data entered into the database, including electronic case report forms (eCRFs), radiation treatment plans and imaging data, will only be transmitted in pseudonymized form. Ancillary and post-trial care: The insurance costs will be covered by the sponsor. Local insurance will be arranged in accordance with local regulations, where applicable. Policy Number: 14.970.888. Dissemination policy: Responsibility for the publication of the results lies with the project management. Until this time, all information on the research project must be treated confidentially. The final publication is planned for after the end of the project. All participating centers will be included in the publication, either as named authors or to the extent that the number of possible co-authors allows. Authors agree to make data and materials supporting the results or analyses presented in their paper available upon reasonable request. Competing interests: J.L. declares Speaker fee from Accuary and Traveling costs from Micropos Medical and from RaySearch Laboratories. The remaining authors declare no conflict of interest.
Figures
References
-
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin Jan. 2023;73(1):17–48. 10.3322/caac.21763. - PubMed
-
- Schaeffer EM, Srinivas S, Adra N, et al. Prostate cancer, version 4.2023, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw Oct. 2023;21(10):1067–96. 10.6004/jnccn.2023.0050. - PubMed
-
- Parker C, Castro E, Fizazi K, et al. Prostate cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol Sep. 2020;31(9):1119–34. 10.1016/j.annonc.2020.06.011. - PubMed
-
- Hamdy FC, Donovan JL, Lane JA, et al. Fifteen-Year outcomes after monitoring, surgery, or radiotherapy for prostate Cancer. N Engl J Med Apr. 2023;27(17):1547–58. 10.1056/NEJMoa2214122. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
